
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- v.3(5); 2017 May

Dietary diversity and child malnutrition in Ghana
Raymond boadi frempong.
a Bayreuth International Graduate School of African Studies, University of Bayreuth, Germany
Samuel Kobina Annim
b Department of Economics, University of Cape Coast, Ghana
The health of children in Ghana has improved in recent years. However, the current prevalence rates of malnutrition remain above internationally acceptable levels. This study, therefore, revisits the determinants of child health by using Ghana’s Multiple Indicator Cluster Survey to investigate the effect of infant feeding practices on child health. We used the World Health Organization’s Infant and Young Children Feeding guidelines to measure dietary quality. The econometric analyses show that dietary diversity may cause improvement in children’s health in Ghana. This suggests that educational campaigns on proper infant feeding and complementary dieting could be an effective means of improving the health of children in Ghana.
1. Introduction
The importance of nutrition has been emphasized for the intellectual and physical development of children. It is, therefore, important to ensure that children have adequate diet as it will ensure a healthy and productive population in future. The benefits of adequate nutrition to the economy come directly in the form of reduced public health expenditure on health care and indirectly through improved health, which may lead to economic growth ( Hoddinott et al., 2008 ). Because of the importance of nutrition in human and economic development, pragmatic steps, both at sub-national, national and international levels, have been taken to reduce the incidence of malnutrition. The importance development practitioners attach to nutrition is reflected in targets 1C and 4A of the first Millennium Development Goal’s (MDG), which identify the need to reduce hunger and mortality among children under five years of age. In spite of the various interventions, about 870 million people were malnourished globally between 2010 and 2012 (FAO, 2012), with a sizeable proportion of this is found in sub-Saharan Africa and Asia ( UNICEF, WHO & World Bank, 2015 ). Also, women and children tend to be the most affected ( Bain et al., 2013 ). According to UNICEF, WHO & World Bank’s (2016) joint child malnutrition estimates, about 32 percent of children in Africa are stunted whilst another 8 percent are wasting. Malnutrition at the early stages of life does not only affect health outcomes of the child, but it also has a serious adverse impact on the determinants of their livelihoods, such as physical and intellectual growth, school performance and eventual future earnings and productivity ( Hoddinott et al., 2008 ; Strauss and Thomas, 1998 ). As individuals get locked up in a vicious cycle of poor health, lower learning capacity, reduced physical activity, and lower productivity as a result of poverty, malnutrition and poor child health nexus, the gains from previous economic growth may be threatened ( Bagriansky, 2010 ).
Some countries in Africa, including Ghana, have made marginal, but steady, gains in reducing malnutrition among children less than five years ( ICF Macro, 2010 ). However, according to the last Multiple Indicator Cluster Survey (MICS4), 13 percent of children in Ghana are moderately or severely underweight, 23 percent are stunted (too short for their age.), and 6 percent are wasting (too thin for their height.) ( Ghana Statistical Service (GSS), 2011 ). Fig. 1 presents the nutritional status of children according to the Ghana Demographic Health Survey (GDHS, rounds I −V) and MICS4. The graph shows varying trends for overweight, stunting, underweight and wasting among children aged 5 to 59 months in Ghana. The graph shows that child stunting and underweight have reduced since 2003, even though the proportion of children who are stunted in Ghana is still higher than the global average of 25 percent ( UNICEF, 2013 ). On the other hand, child wasting and overweight rose between 2003 and 2008. Both indicators increased by 1 percent between 2003 and 2008. Similarly, the GDHS estimate of child wasting is higher than the global estimate of five (5) percent ( UNICEF, 2013 ). Whilst these figures are encouraging when they are benchmarked against other African countries ( UNICEF, WHO & World Bank, 2016 ), they are still above the World Health Organization’s (WHO) classification of low prevalence. Thus, notwithstanding this progress, there is the need to investigate the drivers behind malnutrition in Ghana. This has become necessary given the fact that there has not been a steady downward trend for some indicators.

Nutritional Status of Children under Five Years in Ghana from the GDHS I–V and Ghana MICS-4. (Source: ICF Macro (2010) and GSS (2011) ).
Following UNICEF’s (1990) conceptual framework on the causes of malnutrition, researchers have attempted to explain the role of quality diet in reducing child malnutrition. The empirical literature is replete with the assessment of complementary feeding and its effect on children’s health and nutrition ( Dewey and Adu-Afarwuah, 2008 ; Saha et al., 2008 and Vaahtera et al., 2001 ). The results from these studies suggest that proper complementary feeding could be effective in improving the health of children below the age of five years. In line with these findings, this paper studies the effect of dietary diversity as means of improving child health in Ghana.
Whilst UNICEF’s (1990) conceptual framework links food security to child nutrition, the relationship is not as simple as demonstrated by the framework. Given the fact that food security as a concept is multifaceted, the transmission mechanism of food security to better nutrition can either run from food availability in terms of quantity and quality or sustainability. Thus, policy intervention aimed at improving nutrition through food security may have different impacts, based on which aspect is targeted. In addition, the relationship between food security and child nutrition could be more complex, based on the level of the analysis and the interactions of social, environmental and cultural practices. Government policy can improve child nutrition by ensuring food security at the household or at the individual (child and mother) level. However, depending on which level is targeted, the transmission mechanism will differ and the desired impact may be achieved at different time intervals. In view of these complexities, the current study seeks to test the hypothesis that the consumption of a diversified diet leads to better child nutrition. To the best of our knowledge, this study is different from other studies conducted on the subject to the extent that we take care of the endogeneity between dietary diversity and child health outcomes.
The next section of the paper discusses the methodology, then we present results and discussion and finally draw conclusions from the study.
2. Methodology
Data for the study was obtained from the fourth round of the Ghana Multiple Indicator Cluster Survey (MICS4) collected in 2011. The MICS4 was conducted by the GSS as part of a broader international household survey designed by the UNICEF. The aim of the survey is to provide current information on the socio-economic circumstances of children and women by measuring key indicators relating to the MDGS ( GSS, 2011 ). MICS4 is, therefore, a cross-sectional survey that provides current information on the health, social and economic circumstances of women, children and other household members. To obtain the sample for the survey, rural and urban areas in the ten administrative regions of Ghana were used as the main sampling strata. The final sample was selected in two stages. In the first stage, enumeration areas were selected with the probability of selection being proportional to the size. Then 15 households in each enumeration area were systematically selected. Eventually, 12,150 households were successfully sampled and interviewed. This consists of 11,925 households, 10,627 women aged 15 to 49 year and 7550 under the age of five years ( GSS, 2011 ). After cleaning a merging the various data files, we 6598 children remained for the regression analysis.
2.2. Measurement of dietary diversity
To measure dietary quality, we adopt the WHO’s Infant and Young Children Feeding guidelines (IYCF), because they are designed to measure dietary diversity for both breastfed and non-breastfed children. Also, the dataset used in the analysis contains information on the food items that can be used to calculate this indicator. The section of the survey on children collected information on food and liquids a child consumed in the previous day. We categorized these food items into seven major food groups based on the WHO’s IYCF guidelines ( Swindale and Bilinsky, 2006 ). These food groups are: (i) grains, roots, and tubers; (ii) legumes and nuts; (iii) flesh foods (meat, fish, poultry and liver/organ meats); (iv) eggs; (v) vitamin A rich fruits and vegetables; (vi) dairy products (milk, yogurt, cheese); (vii) other fruits and vegetables. If a child consumed at least one food item from a food group, the group was assigned a value of one for that child. The group scores are then summed to obtain the dietary diversity score, which ranges from zero to seven, where zero represents non-consumption of any of the food items and seven represents the highest level of diet diversification.
2.3. Definition of nutrition status (anthropometric indicators)
In this study, the child’s nutritional status is measured by the WHO’s (2006) anthropometric indicators: height-for-age (HAZ) is used to measure chronic malnutrition due to prolonged food deprivation; weight-for-height (WHZ) captures undernutrition due to recent food deprivation and malnutrition. Weight-for-age which is measures the child’s body mass relative to her chronologic age is used as a proxy for underweight.
2.4. Model specification and estimation technique
Based on the reviewed literature and the objective of this study we estimate the following model:
where: sex = sex of child; age = age of child; numchildren = number of children in household; urban = whether household is in an urban area; mage = mother ’ s age; medu = mother ’ s education; wealth = wealth quintile; water = source of water; toilet = type of toilet; food = food diversity score; Bmilk = child ever breastfed; ethnic = ethnicity of household head; region = which administrative region household is located in; y j = ( W A Z , H A Z , W H Z ) are the raw z-score of the respective indicator; and i indexes individual children .
Estimating Eq. (1) with ordinary least squares (OLS) can yield a consistent estimate of the effect of dietary diversity on child health if dietary diversity is exogenous; that is uncorrelated with the error term in the model. However, this may not be the case because of the bi-causal relationship between the two variables. This bi-causal relationship is likely to arise because parents and caregivers may adopt different feeding practices depending on the current health status of the child. In this instance, the direction of causality could also run from child health to dietary diversity. If this is the case, the OLS estimates will no longer be consistent. To resolve this problem, we employed the Two Stage Least Square (TSLS) estimator to identify the causal effect of dietary diversity on child health. We used the number of chicken owned as well as household ownership of pigs as instruments for dietary diversity. We assume our instruments have no direct effect on child health outcomes but they indirectly influence it by improving the quality of diet consumed. Based on these considerations we estimate the following equations:
where f o o d i ˆ is the linearly predicted food diversity score from Eq. (2) ; pig and chicken are the number of pigs and chicken owner by the household.
3. Results and discussion
Table 1 presents the bivariate relationship between children’s nutritional outcomes, on the one hand, and individual and household characteristics, on the other hand. We find that approximately 25 percent of male children are stunted as compared to 20 percent of females. Similarly, 7.6 percent and 15.6 percent of male children are wasted and considered underweight respectively, whilst 5.2 and 11 percent of female children are wasted and underweight. In all cases, the incidence of malnutrition tends to be higher among male children than female children. This situation could be attributed to differences in biological composition and caregiving; and possibly due to daughter preference ( Fuse, 2010 ).
Bivariate analysis of socioeconomic variables and anthropometric indicators.
Source: Authors’ Computation from MICS4, 2011 .
One can also observe that the difference between the incidence of malnutrition over the different age groups is statistically significant. It is important to note that in all the three cases the proportion of malnourished children increases with age up to age 35 months and then falls, thus, suggesting a non-linear relationship between child age and nutritional status. Apart from stunting, we observe significant differences in the prevalence of wasting and underweight among children who had suffered from fever in the past two weeks and those who had not.
On the association between dietary diversity and child health, Table 1 shows that malnourishment varies significantly for the different levels of consumption. About a quarter of children who consumed at least four of the seven food items are stunted: 5 percent of this group were wasted and another 12 percent were underweight. The prevalence of wasting and child underweight begins to decline after the intake of two or more food items. Thus, child health improves as the intensity of dietary diversity increases.
Sanitation factors such as the type of toilet facility and the source of drinking water also tend to have a significant association with child health in Ghana. About 30 percent of children found in households where the bush or bucket are used as toilet facility is stunted, whilst only 10 percent of their counterparts in households with flush toilets are stunted. Similarly, only 4 percent of children found in households with flush toilets are wasted as compared to 7 percent of children found in households which neither use flush toilet nor pit latrine. The incidence of malnutrition decreases as the source of drinking water improves. For instance, the prevalence of child underweight falls from 17 percent among those who use unprotected water sources to 11 percent among those who use pipe-borne water. Good sanitation and water supply improve health by reducing infections and malnutrition ( Cuesta, 2007 ).
We also find that wealthier households have children with better nutritional status than poorer households. About a third of children born to poor parents are stunted. Equally, one-fifth of children born into poor households are underweight compared to only 6 percent of those in the richest households. A similar pattern was observed by Urke et al. (2011) , who found that wealth status and maternal education are positively associated with child health outcomes. In addition, we observe a positive relationship between maternal education and child health outcomes. The effect of dependence and competition for care is also felt through the number of children in the household. Table 1 shows that child nutritional status worsens as the number of children increases. This could be because of competition for care and resources in the household.
3.1. Feeding pattern in Ghana by child age groups
Fig. 2 provides a description of dietary diversity across different child age groups and it shows that in Ghana a majority of children (47%) consume a minimum of four out of the seven food groups. About a quarter of them had three food groups whilst 13 percent had none of the food groups. In addition, more than 80 percent of infants, aged zero to five months, can be assumed to be undergoing exclusive breastfeeding since they consumed none of the food items. Observable from Fig. 2 is how food diversity increases with child age. For instance, whilst only 0.5 percent of children who are under 6 months of age had at least four of the food items, the proportions increased to 49 percent among those aged 12 to 23 months and 61 percent among those aged 48 to 59 months. The pattern portrayed by this graph indicates that parents and caregivers see the need to vary their children’s diet within the first five years.

Feeding Pattern in Ghana by child age groups. (Source: Authors’ Computation from MICS, 2011).
3.2. Maternal education and food diversity
In Table 2 we test whether dietary diversity for children is statistically different across levels of maternal education. The table shows that children born to parents with higher levels of education had a more diversified diet. We found that children whose mothers have primary, middle/Junior High School (JHS) or at least secondary school education are significantly likely to consume more diversified diet than those whose mothers have no education. However, we fail to find any statistical difference in child feeding among those whose parents had received some form of formal education. Thus, as far as child feeding is concerned the feeding pattern of children who are born to parents with only primary education is not statistically different from those who are born to mothers with either middle/JHS or secondary school education. This suggests that intensifying nutrition education at basic/primary school level could also be an effective approach to fighting malnutrition.
Dietary diversity across levels of maternal education.
+ p < 0.1, * p < 0.05, ** p < 0.01, *** p < 0.001. Source: Authors’ Computation from MICS, 2011 .
3.3. Regional distribution of food diversity among children under 6 years
In terms of regional differences in dietary pattern, Fig. 3 shows that children in the Volta region had the most diversified diet. This is followed by Greater Accra, which is the national capital. One would have expected regions like Eastern and Western to have better food diversity than Upper West and Upper East regions since the poverty rates in the former are lower than the latter region; however, the graph portrays a different picture. This could be as a result of the fact that most of the households in the Upper East and West regions are peasant farmers who grow a wide range of crops and, rear different domestic animals which serve to improve dietary diversity. The average dietary diversity of children in the Northern, Western and Eastern regions are less than the national average of 3.12. The implication of this of this pattern on children’s nutrition is seen in Table 1 , where the regions with low dietary diversity are also the ones with a high incidence of child malnutrition.

Distribution of Food Diversity by Administrative Regions in Ghana. (Source: Authors’Computation from MICS, 2011).
3.4. Estimation results
This paper set out to study the effects of dietary diversity on child health outcomes. To this end, anthropometric indicators of child health were regressed on dietary diversity, maternal education, ethnicity and other covariates of child health. The OLS and TSLS result of the effect of dietary diversity on child anthropometric indicators are presented in Table 3 . The first stage results for the TSLS are reported in column 7. Table 3 indicates that dietary diversity has a positive effect on child health outcomes. This relationship is observed in all the models, except for the IV model for weight-for-age. Thus, Increasing the number of food groups a child consumes by one causes HAZ and WAZ to increase by 0.65 and 0.52 units respectively. Thus, we find a consistent positive association between dietary diversity and better child health outcomes.
Effects of food diversity, mother's education and ethnicity on child health outcomes in Ghana (all children under 5 years).
On the effect of ethnicity on child health, we find in Table 3 that children from the Ewe, Grusi, Guan and Mole/Dagbani ethnic groups have better anthropometric scores than those from the Akan ethnic group. This result shows that ethnicity may have an important influence on child health in Ghana. This may be attributed to differences in feeding and post-partum practices across the different ethnic groups. Elsewhere, Adedini et al. (2015) and Annim and Imai (2014) have found that child health outcomes differ among children of different ethnic descent in Lao People’s Democratic Republic.
We also observe that an increase in the number of children in the household worsens the child's health. The table shows that an additional child in the household is associated with a 0.2 lower WHZ and a 0.3 lower scores in both WAZ and HAZ. Annim, Awusabo-Asare, Amo-Adjei (2013) argued that as the number of children in a household increase, children may have to compete for both household resources and caregiving. This may cause each child to receive sub-optimal care and resources to achieve the desired nutritional status. In line with our observation in Table 1 , male children tend to have lower weight-for-age and height-for-age than their female counterparts. The observed relationship between sex and nutritional status could be because of biological differences as well as socio-cultural differences. Socio-culturally, gender preferences, and preferential treatment may account for the observed coefficient. Indeed, Fuse (2010) has shown that daughter preference is slightly higher than son preference in Ghana.
In addition, children who had diarrhea have lower anthropometric scores compared to those who did not. Infections that lead to diarrhea and fever adversely affect nutritional status by reducing dietary intake and intestinal absorption and increasing catabolism and sequestration of nutrients which are essential for growth ( Brown, 2003 ). However, we fail to see this effect in the case of HAZ for children who had a fever. We also observe a negative relationship between child’s age and nutritional status.
As expected, household wealth positively correlates with height-for-age and weight-for-height. Children born to families within higher wealth quintiles tend to have better nutritional status as compared to those born to households within the poorest wealth quintile. For HAZ and WAZ, the effect of household wealth and child nutritional status falls between those in the second and middle quintiles but increases between the fourth and the richest quintiles. This suggests that the relationship between wealth and child health may not be linear. Conversely, weight-for-height is worse among children in the second and middle wealth quintiles as compared to those in the poorest wealth quintile.
Regional fixed effects are significant in explaining child nutrition. With the Western region as the base, we observe that except for Greater Accra, children in the other regions have lower weight-for-age than those in the Western region. Similarly, children in Northern, Upper East, and Upper West regions are worse off in terms of weight-for-height than their counterparts in the Western region. Interestingly the difference between the anthropometric score of children in the Western region and the three northern regions tends to be higher. This could be attributable to the high poverty and deprivation rates in this region.
3.5. Proportional selection assumption test
Following Oster (Oster, 2014) we test whether the omission of unobservable factors may significantly bias the observed coefficients of dietary diversity in our models. The test assumes that an inference can be made about the possible bias that could be caused by the omission of unobservable factors by observing the movement of the coefficient by successively including observable independent variables. The idea of the test is that if the inclusion of additional explanatory variables improves the R 2 but leaves the coefficient relatively unchanged, then one can be confident that the coefficient is relatively stable. Based on this, it can be concluded that the coefficient will remain relatively unchanged if the unobservable factors were added. Table 4 contains the results of the test. We select an R 2 cutoff of 30 percent, because studies in this are usually report R 2 around 20 percent (see Arimond and Ruel (2004) for a cross country study and the respective R 2 ). We found that, except for the WHZ model, the identified set always excludes zero. This is means that even though these models do not include all the potential explanatory variables, the effect of dietary diversity will be different from zero if we were to observe these variables.
Proportional Selection Assumption.
δ = 1 , R m a x 2 = 3 .
4. Discussion and conclusion
Because of the long-lasting effect of malnutrition on human development at later stages in life, children’s nutrition has engaged the attention of policy makers and researcher for several years. This has led to the prescription of various interventions to deal with child malnutrition, of which dietary diversity is an integral part. The association between dietary diversity and child health outcomes has been explored by researchers in some developing countries. In view of the evidence from these studies, the current study sought to investigate the causal effect of dietary diversity on child health outcomes in Ghana.
Food diversity, the independent variable of interest, was captured as a continuous variable from the count of the number of food groups from which a child had food in the previous day before the survey. These food groups are based on the WHO’s IYCF guidelines. The dependent variable, child health, was measured with three anthropometric indicators: weight-for-age (wasting), weight-for-height (stunting) and weight-for-height (underweight). We employed both bivariate and multivariate analyses to evaluate the effect of dietary diversity on child health. We found that there is a general trend towards higher dietary diversity as the child grows in age. We consider this as a good trend for child nutrition, as parents and caregivers see the need to meet the nutritional requirements of their wards in the growth process. Dietary diversity is also significantly higher for children from mothers with higher education. This was consistent with our apriori expectation since educated mothers know the importance of a balanced diet for their children. This also puts education as one of the important tools that policy makers can adopt to improve nutritional adequacy among infants and young children. This can be achieved by making nutrition awareness an integral part of the school curriculum, especially at the basic level. Since more than half of the respondents in our sample had had no formal education, we recommend that nutrition awareness should also be created outside the classroom through avenues like the mass media and informal education. The government of Ghana can take advantage of the existing information service department as well the flourishing community information centers to provide informal education on nutrition, especially in rural Ghana.
In general, our analysis shows that dietary diversity causes improvements in child health among under five-year-olds in Ghana. We interpret this results with caution because dietary diversity was measured over a one-day recall period which may not be an accurate reflection the dietary pattern for a longer period. Despite this limitation, our results show a consistent relationship across all the three anthropometric indicators. We recommend that public health officials should educate parents and caregivers on the importance of dietary diversity to their children. The government could also take advantage of the structures of the national school feeding program to diversify the diet of the school children. Our analysis of the effects of each individual food groups on child health shows that vitamin A rich food (pumpkin, yellow yam, green vegetables [kontomire] mangoes and pawpaw), eggs and other vegetables have a positive association with the weight-for-age score. Hence, given the right nutritional education, malnutrition among children in rural areas could be minimized at a relatively lower cost because these food items tend to be inexpensive in rural farming communities.
Declarations
Author contribution statement.
Raymond Boadi Frempong, Samuel Kobina Annim: Conceived and designed the experiments; Performed the experiments; Analyzed and interpreted the data; Contributed reagents, materials, analysis tools or data; Wrote the paper.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interest statement
The authors declare no conflict of interest.
Additional information
No additional information is available for this paper.
- Adedini S.A., Odimegwu C., Imasiku E.N., Ononokpono D.N. Ethnic differentials in under-five mortality in Nigeria. Ethn. Health. 2015; 20 (2):145–162. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Annim S.K., Imai K.S. Nutritional Status of Children. Food Consumption Diversity and Ethnicity in Lao PDR. 2014 (No. DP2014-17) [ Google Scholar ]
- Annim S.K., Awusabo-Asare K., Amo-Adjei J., ICF International Household Nucleation, Dependency and Child Health Outcomes in Ghana. DHS Working Papers. August 2013 http://www.measuredhs.com/publications/publication-wp98-working-papers.cfm [ PubMed ] [ Google Scholar ]
- Arimond M., Ruel M.T. Dietary diversity is associated with child nutritional status: evidence from 11 demographic and health surveys. J. Nutr. 2004; 134 (10):2579–2585. [ PubMed ] [ Google Scholar ]
- Bagriansky J. UNICEF; Albania: 2010. The economics consequences of malnutrition in Albania. [ Google Scholar ]
- Bain L.E., Awah P.K., Geraldine N., Kindong N.P., Sigal Y., Bernard N., Tanjeko A.T. Malnutrition in Sub − Saharan Africa: burden, causes, and prospects. Pan Afr. Med. J. 2013; 15 :120. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Brown K.H. Diarrhea and Malnutrition. J. Nutr. 2003; 133 (1):328S–332S. [ PubMed ] [ Google Scholar ]
- Cuesta J. Child Malnutrition and the Provision of Water and Sanitation in the Philippines. Journal of the Asia Pacific Economy. 2007; 12 (2):125–157. [ Google Scholar ]
- Dewey K.G., Adu-Afarwuah S. Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Matern. Child Nutr. 2008; 4 (Suppl. 1):24–85. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Fuse K. Variations in attitudinal gender preferences for children across 50 less-developed countries. Demographic Research. 2010; 23 (36):1031–1048. [ Google Scholar ]
- Ghana Statistical Service . Ghana Statistical Service; Accra, Ghana: 2011. Ghana Multiple Indicator Cluster Survey with an Enhanced Malaria Module and Biomarker, (Final Report) [ Google Scholar ]
- Hoddinott J., Maluccio J.A., Behrman J.R., Flores R., Martorell R. Effect of a nutrition intervention during early childhood on economic productivity in Guatemalan adults. Lancet. 2008; 371 (9610):411–416. [ PubMed ] [ Google Scholar ]
- ICF Macro . ICF Macro; 2010. Trends in demographic, family planning, and health indicators in Ghana, 1960-2008: Trend analysis of demographic and health surveys data. [ Google Scholar ]
- Saha K.K., Frongillo E.A., Alam D.S., Arifeen S.E., Persson L.Å., Rasmussen K.M. Appropriate infant feeding practices result in better growth of infants and young children in rural Bangladesh. Am. J. Clin. Nutr. 2008; 87 (6):1852–1859. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Strauss J., Thomas D. Health, nutrition, and economic development. J. Econ. Lit. 1998; 36 (2):766–817. [ Google Scholar ]
- Swindale A., Bilinsky P. Food and Nutrition Technical Assistance Project, Academy for Educational Development; Washington, DC: 2006. Household dietary diversity score (HDDS) for measurement of household food access: indicator guide. [ Google Scholar ]
- UNICEF . UNICEF; New York: 2013. Improving child nutrition: The achievable imperative for global progress. [ Google Scholar ]
- UNICEF, WHO, World Bank . Global Database on Child Growth and Malnutrition; 2015. Levels and trends in child malnutrition: Key findings of the 2015 edition. [ Google Scholar ]
- UNICEF, WHO, World Bank . Global Database on Child Growth and Malnutrition; 2016. Levels and trends in child malnutrition: Key findings of the 2016 edition. [ Google Scholar ]
- Urke H.B., Bull T., Mittelmark M.B. Socioeconomic status and chronic child malnutrition: Wealth and maternal education matter more in the Peruvian Andes than nationally. Nutr. Res. 2011; 31 (10):741–747. [ PubMed ] [ Google Scholar ]
- Vaahtera M., Kulmala T., Hietanen A., Ndekha M., Cullinan T., Salin M.L., Ashorn P. Breastfeeding and complementary feeding practices in rural Malawi. Acta Paediatr. 2001; 90 (3):328–332. [ PubMed ] [ Google Scholar ]
- Open access
- Published: 28 November 2007
Malnutrition and the disproportional burden on the poor: the case of Ghana
- Ellen Van de Poel 1 , 2 ,
- Ahmad Reza Hosseinpoor 3 ,
- Caroline Jehu-Appiah 4 ,
- Jeanette Vega 3 &
- Niko Speybroeck 5
International Journal for Equity in Health volume 6 , Article number: 21 ( 2007 ) Cite this article
30k Accesses
73 Citations
6 Altmetric
Metrics details
Malnutrition is a major public health and development concern in the developing world and in poor communities within these regions. Understanding the nature and determinants of socioeconomic inequality in malnutrition is essential in contemplating the health of populations in developing countries and in targeting resources appropriately to raise the health of the poor and most vulnerable groups.
This paper uses a concentration index to summarize inequality in children's height-for-age z-scores in Ghana across the entire socioeconomic distribution and decomposes this inequality into different contributing factors. Data is used from the Ghana 2003 Demographic and Health Survey.
The results show that malnutrition is related to poverty, maternal education, health care and family planning and regional characteristics. Socioeconomic inequality in malnutrition is mainly associated with poverty, health care use and regional disparities. Although average malnutrition is higher using the new growth standards recently released by the World Health Organization, socioeconomic inequality and the associated factors are robust to the change of reference population.
Child malnutrition in Ghana is a multisectoral problem. The factors associated with average malnutrition rates are not necessarily the same as those associated with socioeconomic inequality in malnutrition.
In the developing world, an estimated 230 million (39%) children under the age of five are chronically malnourished and about 54% of deaths among children younger than 5 are associated with malnutrition [ 1 ]. Malnutrition is a major public health and development concern with important health and socioeconomic consequences. In Sub-Saharan Africa, the prevalence of malnutrition among the group of under-fives is estimated at 41% [ 1 ]. It is the only region in the world where the number of child deaths is increasing and in which food insecurity and absolute poverty are expected to increase [ 2 – 4 ]. Malnutrition in early childhood is associated with significant functional impairment in adult life, reduced work capacity and decreasing economic productivity [ 5 – 10 ]. Children who are malnourished not only tend to have increased morbidity and mortality but are also more prone to suffer from delayed mental development, poor school performance and reduced intellectual achievement [ 6 – 8 ].
Chronic malnutrition is usually measured in terms of growth retardation. It is widely accepted that children across the world have much the same growth potential, at least to seven years of age. Environmental factors, diseases, inadequate diet, and the handicaps of poverty appear to be far more important than genetic predisposition in producing deviations from the reference. These conditions, in turn, are closely linked to overall standards of living and the ability of populations to meet their basic needs. Therefore, the assessment of growth not only serves as one of the best global indicators of children's nutritional status, but also provides an indirect measurement of the quality of life of an entire population [ 11 – 13 ].
Large scale development programs such as the Millennium Development Goals (MDGs) have also emphasized the importance of the under-fives' nutritional status as indicators for evaluating progress [ 14 ]. When aiming at reducing childhood malnutrition, it is important not only to consider averages, which can obscure large inequalities across socioeconomic groups. Failure to tackle these inequalities may act as a brake on making progress towards achieving the MDGs and is a cause of social injustice [ 15 , 16 ].
Against this background, Ghana provides an interesting case study. The country experienced remarkable gains in health from the immediate post independence era. Life expectancy improved over the years and the prevention of a range of communicable diseases improved child survival and development. However in the last decade despite increasing investments in health, Ghana has not achieved target health outcomes. There has been no significant change in Ghana's under-five and infant mortality rates between 1993 and 2003. In the last couple of years, under-five mortality was actually slightly increasing. Life expectancy has also fallen from 57 years in 2000 to 56 years in 2005 [ 17 ]. Ghana's Human Development Index (HDI), a measure combing life expectancy, literacy, education and standard of living, has been worsening too; after improving from 0.444 in 1975 to 0.563 in 2001, the HDI dropped to 0.520 in 2005 [ 15 ]. Since 1988, there has been no definite trend in malnutrition (in terms of height-for-age). Apparent gains between 1988 and 1998 were reversed in 2003 [ 18 ]. Although the 2003 Ghana Demographic Health Survey (DHS) final report [ 17 ] recommends caution when using data from the various DHS to assess the trend in the nutritional status, it is noted that there was a trend over the past five years of increased stunting compared to a decrease of wasting and underweight. Further, there has been a trend of continued high values of stunting in the North compared to the South [ 17 , 19 ].
Malnutrition in Ghana has been most prevalent under the form of Protein Energy Malnutrition (PEM), which causes growth retardation and underweight. About 54% of all deaths beyond early infancy were associated with PEM, making this the single greatest cause of child mortality in Ghana [ 20 ].
A paradigm shift in Ghanaian health policy has been taking place in 2006. The theme for the new health policy in Ghana was 'Creating Wealth through Health". One of the fundamental hypotheses of this policy was that improving health and nutritional status of the population would lead to improved productivity, economic development and wealth creation [ 21 ]. Since this policy adopted an approach that addressed the broader determinants of health, it has thus generated interest in socio-economic inequalities in health and malnutrition. It was further recognised that not paying attention to malnutrition inequalities during the early years of life is likely to perpetuate inequality and ill health in future generations and thus defeat the aims of the new health policy.
From the existing evidence it is clear that childhood malnutrition is associated with a number of socioeconomic and environmental characteristics such as poverty, parents' education/occupation, sanitation, rural/urban residence and access to health care services. Also demographic factors such as the child's age and sex, birth interval and mother's age at birth have been linked with malnutrition [ 4 , 5 , 22 – 26 ]. Previous studies have also drawn attention to the disproportional burden of malnutrition among children from poor households [ 27 – 31 ]. However, much less is known on which factors lie behind this disproportional burden. It is important to note that the most important determinants of malnutrition are not necessarily also the most important determinants of socioeconomic inequality in malnutrition. [ 31 ] shows that the poorest-to-richest odds-ratio of stunting is almost halved by controlling for household and child characteristics using Ghanaian data. However, it is not clear how much each of these characteristics is contributing to this reduction. Understanding the nature and determinants of socioeconomic inequality in malnutrition is essential in contemplating the health of populations in developing countries and in targeting resources appropriately to raise the health of the poor and most vulnerable groups. This paper employs a concentration index to summarize inequality across the entire socioeconomic distribution rather than simply comparing extremes as in ratio measures. The concentration index is decomposed using the framework suggested by [ 32 ], allowing to identify the factors that are associated with socioeconomic inequality in malnutrition. This decomposition takes into account that both the association of a determinant with malnutrition as well as its distribution across socioeconomic groups play a role in the extent to which it is contributing to socioeconomic inequality in malnutrition. The usefulness of this approach has already been demonstrated on European data, but has known limited applications on developing countries.
Further, this paper contributes to the literature by delivering evidence on the determinants of malnutrition and socioeconomic inequality in Ghana using the new child growth standards population that has recently been released by the World Health Organization (WHO) [ 33 ]. This reference population includes children from Brazil, Ghana, India, Norway, Oman and the US. The new standards adopt a fundamentally prescriptive approach designed to describe how all children should grow rather than merely describing how children grew in a single reference population at a specified time [ 34 ]. For example, the new reference population includes only children from study sites where at least 20% of women are willing to follow breastfeeding recommendations. To our knowledge this is the first study presenting estimates of malnutrition in Ghana based upon these new standards. To check sensitivity of the results to this change in reference group, the analysis is also done using the US National Center for Health Statistics (NCHS) reference population [ 35 ].
The results are useful from a policy perspective as they can be used in setting policies to reduce malnutrition and the excessive burden on the poor. The results of this study are particularly relevant for Ghanaian policy makers, but can also be generalized to other settings in the sense that they show that malnutrition is associated with a broad range of factors and that the factors related to average malnutrition are not necessarily the same as those related to socioeconomic inequality in malnutrition.
Measuring malnutrition
Nutritional status was measured by height-for-age z-scores. An overview of other nutritional indices and why height-for-age is the most suited for this kind of analysis is provided in [ 36 ]. A height-for-age z-score is the difference between the height of a child and the median height of a child of the same age and sex in a well-nourished reference population divided by the standard deviation in the reference population. The new WHO child growth population is used as reference population [ 33 ]. To construct height-for-age z-scores based upon these standards, we used the software available on the WHO website [ 37 ]. To check sensitivity of the results to this change in reference group, the analysis is also done by using the US National Center for Health Statistics (NCHS) reference population [ 35 ].
Generally, children whose height-for-age z-score is below minus two standard deviations of the median of the reference population are considered chronically malnourished or stunted. In the regression models, the negative of the z-score is used as dependent variable ( y ). This facilitates interpretation since it has a positive mean and is increasing in malnutrition [ 32 ]. For the purpose of our analysis, using the z-score instead of a binary or ordinal variable indicating whether the child is (moderately/severely) stunted is preferred as it facilitates the interpretation of coefficients and the decomposition of socioeconomic inequality. However, binary indicators of stunting are also used in the descriptive analysis and to position Ghana within a set of other Sub-Saharan African countries.
The concentration index as a measure of socioeconomic inequality
Assume y i is the negative of the height-for-age z-score of child i . The concentration index (C) of y results from a concentration curve, which plots the cumulative proportion of children, ranked by socioeconomic status, against the cumulative proportion of y . The concentration curve lies above the diagonal if y is larger among the poorer children and vice versa. The further the curve lies from the diagonal, the higher the socioeconomic inequality in nutritional status. A concentration index is a measure of this inequality and is defined as twice the area between the concentration curve and the diagonal. If children with low socioeconomic status suffer more malnutrition than their better off peers the concentration index will be negative [ 38 ]. It should be noted that the concentration index is not bounded within the range of [-1,1] if the health variable of interest takes negative, as well as positive values. Since children with a negative y are better off than children in the reference population, they cannot be considered malnourished. Therefore their z-score is changed into zero, such that the z-scores are restricted to positive values with zero indicating no malnutrition and higher z-scores indicating more severe malnutrition.
Further, the bounds of the concentration index depend upon the mean of the indicator when applied to binary indicators, such as stunting [ 39 ]. This would impede cross-country comparisons due to substantial differences in means across countries. To avoid this problem, we used an alternative but related concentration index that was recently introduced by [ 40 ] and does not suffer from mean dependence, when comparing Ghana with other Sub-Saharan African countries.
Decomposition of socioeconomic inequality
More formally, a concentration index of y can be written as [ 38 ]:
where y i refers to the height-for-age of the i -th individual and R i is its respective fractional rank in the socioeconomic distribution. As will be discussed further in the following section, the present paper uses a continuous wealth variable, developed by principal component analysis, as a measure of socioeconomic status [see e.g. [ 41 ]].
If y i is linearly modelled
[ 32 ] showed that the concentration index of height-for-age can be decomposed into inequality in the determinants of height-for-age as follows:
where μ is the mean of y , x ¯ k MathType@MTEF@5@5@+=feaafiart1ev1aaatCvAUfKttLearuWrP9MDH5MBPbIqV92AaeXatLxBI9gBaebbnrfifHhDYfgasaacPC6xNi=xH8viVGI8Gi=hEeeu0xXdbba9frFj0xb9qqpG0dXdb9aspeI8k8fiI+fsY=rqGqVepae9pg0db9vqaiVgFr0xfr=xfr=xc9adbaqaaeGacaGaaiaabeqaaeqabiWaaaGcbaGafmiEaGNbaebadaWgaaWcbaGaem4AaSgabeaaaaa@2EEF@ is the mean of x k , C k is the concentration index of x k (with respect to socioeconomic status) and GCε is the generalized concentration index of the residuals. The latter term reflects the socioeconomic inequality in height-for-age that is left unexplained by the model and is calculated as G C ε = 2 n ∑ i = 1 n ε i R i MathType@MTEF@5@5@+=feaafiart1ev1aaatCvAUfKttLearuWrP9MDH5MBPbIqV92AaeXatLxBI9gBaebbnrfifHhDYfgasaacPC6xNi=xH8viVGI8Gi=hEeeu0xXdbba9frFj0xb9qqpG0dXdb9aspeI8k8fiI+fsY=rqGqVepae9pg0db9vqaiVgFr0xfr=xfr=xc9adbaqaaeGacaGaaiaabeqaaeqabiWaaaGcbaGaem4raCKaem4qam0aaSbaaSqaaGGaciab=v7aLbqabaGccqGH9aqpjuaGdaWcaaqaaiabikdaYaqaaiabd6gaUbaakmaaqahabaGae8xTdu2aaSbaaSqaaiabdMgaPbqabaGccqWGsbGudaWgaaWcbaGaemyAaKgabeaaaeaacqWGPbqAcqGH9aqpcqaIXaqmaeaacqWGUbGBa0GaeyyeIuoaaaa@40B6@ .
As the DHS data have a hierarchical structure, with children nested in households and households nested within communities, we have also considered using multilevel models to estimate the associations of variables with childhood malnutrition (see e.g. [ 42 ]). Allowing for random effects on the household and/or community level yielded coefficients that were similar to the ones from OLS regression corrected for clustering. Because of this similarity and because the use of multilevel models would complicate the decomposition of socioeconomic inequality in malnutrition, the remainder is based on results from linear regression corrected for clustering on the community level.
All estimation takes account of sample weights (provided with the DHS data). Statistical inference on the decomposition results is obtained through bootstrapping with 3000 replications. The bootstrap procedure takes into account the dependence of observations within clusters.
Data is used from the 2003 Ghana Demographic Health Survey (DHS) and are restricted to children under the age of 5. Anthropometric measures are missing for 12.3% of children in this age group. The final sample contains information on 3061 children. We did examine possible selection problems due to the high proportion of missing observations. A logit model explaining the selection in the sample and a Heckman sample selection model (using different exclusion restrictions) were used to check for this [ 43 ]. Both tests did not reveal large sample selection problems, and coefficients in the Heckman model were very similar to those in the model presented here.
The nutritional status of a child is specified to be a linear function of child-level characteristics such as age, sex, duration of breastfeeding, size at birth; maternal characteristics such as education, mother's age at birth, birth interval, marital status, use of health services, occupation and finally household-level characteristics such as wealth, type of toilet facility, access to safe water, number of under-five children in the household, region and urbanization. We preferred not to include information on the type of toilet and water source into the wealth indicator, as these variables can be expected to have a direct relation with children's growth apart from being correlated with household socioeconomic status [ 44 ].
The explanatory variables are described in the last column of Table 1 . All have well documented relevance in the literature [ 5 , 22 – 26 , 31 , 32 , 45 , 46 ].
No information on mother's nutritional status was included in the set of explanatory variables. Since about 10% of women in the dataset were pregnant at the time of interview, their BMI did not provide an accurate measure of their nutritional status. Furthermore, BMI reflects current nutritional status and may not be relevant for children born 5 years prior to the interview. Inclusion of mother's height-for-age had no significant effect on results.
Summary statistics
In the 2003 DHS data for Ghana, 36% of children under the age of 5 are stunted. Stunting is defined as height-for-age being below minus 2 SD from the median of the reference population. The concentration index for stunting in children under the age of 5 was -0.12 (SD = 0.016). This negative value implies that poor children had a higher probability of being stunted than their better off peers. Using the older NCHS reference study showed a lower prevalence of stunting (29%) and slightly higher socioeconomic inequality (C = -0.15, SD = 0.019).
Figure 1 illustrates the strong socioeconomic inequality in childhood stunting. The stunting rate among the poorest 60 percent was more than twice the rate of children in the richest 20 percent.

Distribution of stunting across wealth quintiles.
Figure 2 shows a comparative picture of stunting and socioeconomic inequality in stunting across the Sub-Saharan African region. Stunting and socioeconomic variables are calculated for each country on DHS data in exactly the same way as is described for the Ghana DHS. Summary statistics of all variables are shown in Table 1 .

Average stunting versus socioeconomic inequality in stunting in under-five children in Sub-Saharan Africa. Data from recent Demographic Health surveys. Stunting is measured using the WHO child growth standards. Concentration index as suggested by [40] is used since it is invariant to the mean of the binary variable.
Determinants of malnutrition
The regression coefficients and their significance are shown in the first column of Table 2 . Note that the dependent variable is increasing in malnutrition, such that a negative coefficient should be interpreted as lowering malnutrition.
Malnutrition increased with the child's age in a non-linear way. Children who were very small at birth had a higher probability to be stunted than children with normal size. Male children were more prone to malnutrition than their female peers. Long duration of breastfeeding is associated with higher malnutrition.
With respect to maternal characteristics, the existence of a short birth interval was significantly increasing malnutrition. Children of women that accessed health services more frequently were less prone to being malnourished. Maternal occupation showed no clear effect. Maternal education and household wealth showed a significant association with childhood malnutrition. The presence of two or more under-five children in the household was negatively associated with the child's nutritional status. Sanitation variables however had no significant association on malnutrition. As compared to the Northern region all regions were associated with lower malnutrition, especially the Accra region. The high regional disparities in malnutrition are further illustrated in Figure 3 . The four most deprived regions in Ghana (Northern, Central, Upper East and Western regions) exhibited the greatest burden of malnutrition.

Inequality in stunting by regions (A) and grouped regions (B) (as in [55]).
Decomposition of socioeconomic inequality in malnutrition
Table 2 also shows the concentration index and the relative contributions of each determinant to socioeconomic inequality in childhood malnutrition. For the ease of interpretation, the last column shows the grouped contribution from the categorical variables. A negative contribution to socioeconomic inequality implies that the respective variable is lowering socioeconomic inequality and vice versa. A variable can contribute to socioeconomic inequality in malnutrition both through its association with malnutrition and through its unequal distribution across wealth groups. The extent to which each of the explanatory variables is unequally distributed across wealth is reflected by its C value. A negative C means that the determinant is more prevalent among poorer households.
Wealth accounted for the major part (31%) of socioeconomic inequality. This part of socioeconomic inequality reflects the direct contribution of wealth. The remainder is the wealth-related inequality in malnutrition through other factors. Important contributors were regional variables (23%) and the use of health care services (18%). The age of the child was contributing negatively to socioeconomic inequality (-8%). This means that the combined effect of its coefficient and its distribution by wealth was lowering socioeconomic inequality in malnutrition. Older children were more likely to be stunted and were more prevalent in higher wealth quintiles. The latter is reflected by the positive and significant C of the variable age > 12 months The contribution of the error term only amounted to about 6%, meaning that the decomposition model functioned well in explaining socioeconomic inequality in malnutrition.
Using the older NCHS reference population gave very similar regression and decomposition results are therefore not discussed (results are available upon request.).
Relative to other Sub-Saharan countries, Ghana appeared to have a rather low level of average stunting, combined with relatively high socioeconomic inequality in stunting. The use of the new WHO child growth standards yielded a higher average stunting rate as compared to the older NCHS reference group. [ 47 ] found the same for Bangladesh, Dominican Republic and a pooled sample of North American and European children. However, the variables associated with malnutrition and socioeconomic inequality were very robust to the change of the reference population.
Malnutrition in Ghanaian children rises with the age of the child, which is confirmed by other studies [ 5 , 25 , 32 ]. The higher prevalence of malnutrition among boys as compared to girls, and the negative association of long breastfeeding have also been established in the literature [ 5 , 22 , 32 , 45 ]. Long duration of breastfeeding may be associated with higher malnutrition because it reflects lack of resources to provide children with adequate nutrition [ 31 ]. It is also possible that children who are breastfed for a long time are more reluctant to eat other foods, as was found by [ 22 ] in their study on a cohort of Ghanaian children.
Short birth intervals and the presence of two or more under-five children in the household, affected childhood growth negatively by placing a heavy burden on the mother's reproductive and nutritional resources, and by increasing competition for the scarce resources within the household [ 22 ]. Children of younger mothers could be more prone to malnutrition because of physiological immaturity and social and psychological stress that come with child bearing at young age [ 48 ].
Maternal education was significantly lowering childhood malnutrition. This may reflect education generating the necessary income to purchase food. However, although education is often suggested to be a measure of social status, the coefficient stayed significant after controlling for household wealth and living conditions. A high level of maternal education could also lower childhood malnutrition through other pathways such as increased awareness of healthy behaviour, sanitation practices and a more equitable sharing of household resources in favour of the children [ 4 , 5 , 49 ].
Sanitation in terms of having a toilet and access to safe water did not significantly affect malnutrition. [ 26 ] also reported this result, but they did find a significant association between sanitation and wasting (which reflects current nutritional status). This might suggest that good sanitation can avoid episodes of diarrhoea and hereby affect current nutritional status, while it may not be sufficient for long term child growth.
The higher levels of malnutrition of the population living in the northern regions of Ghana have already been observed more than a decade ago [ 23 ]. This regional pattern reflects ecological constraints, worse general living conditions and access to public facilities in the Northern regions. In addition, the persistence of this regional inequality can point to an intergenerational effect of malnutrition. Since women who were malnourished as children are more likely to give birth to low-birth-weight children, past prevalence of child malnutrition is likely to have an effect on current prevalence.
The high socioeconomic inequality in childhood malnutrition is -apart from wealth itself-mainly associated with regional characteristics and use of health care services. Wealth was responsible for about one third of the socioeconomic inequality in malnutrition. This means that poorer children were more likely to be malnourished, mainly because of their poverty. The regional contribution results from the fact that poorer children are more likely to live in regions with disadvantageous characteristics. Given the strong regional associations with malnutrition, after controlling for a broad range of socioeconomic and demographic covariates, there must be other important regional aspects. The regional inequality in Ghana originates from both geographical and historical reasons. Much of the North is characterized by lower rainfall, savannah vegetation, periods of severe drought and remote and inaccessible location. Further, the colonial dispensation ensured that northern Ghana was a labor reserve for the southern mines and forest economy and the post-colonial failed to break the established pattern [ 19 ].
Health services use was also responsible for a substantial proportion of socioeconomic inequality in malnutrition. This derives from the combined effect of the positive associations between health services use and childhood growth and the unequal use across socioeconomic groups. The reason for the lower health care use amongst the poor may be due to several barriers including the cost of care, cost of transportation and lower awareness on health promoting behavior [ 50 ]. User fees were introduced in Ghana in 1985 as a cost-sharing mechanism at all public health facilities. To ensure access to health care services for the poor and vulnerable the government introduced fee exemptions. Then again in 2003, a new policy for exempting deliveries from user fees in the four most deprived regions of the country, namely Central, Northern, Upper East and Upper West regions were introduced. To further bridge the inequality a key recommendation of the Ghana Poverty Reduction Strategy [ 51 ] was to allocate 40% of the non-wage recurrent budget to the deprived regions. However, experience to date indicates that Ghana has not been able to implement an efficient exemption mechanism or commit to the 40% budgetary allocation to achieve the principal purpose. In addition to these financial hurdles, poorer people are often also located further from health centers. The ratios of population to nurses and doctors are the highest the poorest regions of Ghana. For example the ratio of population to doctors in the northern region is 1:81338 compared to the national average of 1:17733. Trends show that since 1995 the Northern region has had the lowest average number of outpatient visits per capita in the country [ 52 ]. Also partly related to the use of health services is the contribution of the number of under-fives in the household. Poor women are more likely to have more children and these, in turn, are therefore more likely to be malnourished. The higher parity among poorer women may be related to difficult access to or knowledge on family planning services. The much lower use and knowledge of modern contraception among poor women is documented in the Ghana DHS 2003 final report [ 17 ].
The negative contribution of age comes from the combined facts that older children are more likely to be malnourished and at the same time more prevalent in the richer wealth quintiles. The latter could be related to higher child and infant mortality rates amongst poorer households that cause the proportion of older children to be lower among poor households as compared to richer households.
Combining the results from the analysis on the determinants of malnutrition and socioeconomic inequality demonstrates that variables that are associated with average malnutrition are not necessarily also related to socioeconomic inequality. Although bio-demographic variables such as a risky birth interval, size at birth, duration of breastfeeding and the sex of the child are quite strongly associated with a child's nutritional status, they do not contribute to socioeconomic inequality in malnutrition. This is because of their relatively equal distribution across socioeconomic groups. Other variables such as urban/rural location, having a toilet, access to clean water and maternal occupation are very unequally distributed across socioeconomic groups, but still do not contribute to socioeconomic inequality in malnutrition because they are not significantly associated with malnutrition. A third group of variables such as regions, health care use and wealth are both very strongly related to average and socioeconomic inequality in malnutrition.
Considerations and limitations
There exist some limitations of this study. First, DHS only collects information on the recent food consumption of the youngest child under three years of age living with the mother. Restricting the sample to these children would substantially reduce the number of observations. However, the analysis was also conducted on this sub sample, using food consumption as one of the determinants of malnutrition (indices were created similar to [ 25 , 45 ]). Since the regression and decomposition results did not differ much, these are not presented in this paper (but are available from the authors upon request). Second, one has to bear in mind that, although commonly used, the construction of an asset index to capture socioeconomic status has its shortcomings and e.g. is sensitive to the assets included [ 44 ]. However, in the absence of reliable information on income or expenditure, the use of such an asset index is generally a good alternative to distinguish socioeconomic layers within a population [ 53 ]. Finally, it is important to note that this paper is showing the factors that are associated with malnutrition and socioeconomic inequality in malnutrition and the magnitude of these associations. These results are subject to the usual caveats regarding the causal interpretation of cross-sectional results. Focusing on child health avoids much of the direct feedback of income and health that is usually present in microeconomic studies. To gain some insight into the severity of endogeneity problems we also did the analysis excluding possible endogenous variables such as birth interval, breastfeeding, the number of children in the household and use of health care services. Again, wealth and regional characteristics were contributing most to socioeconomic inequality, followed by maternal education. To avoid endogeneity of health care use, it would be better to use data on proximity/availability of care. However, no such data were available in the 2003 Ghana DHS. Another option would be to predict health care use, but we were not able to find strong predictors for health care.
Conclusion and policy implications
The regression results show that malnutrition is associated with a broad range of factors. However in Ghana it often falls through the cracks since it has no institutional home. Tackling malnutrition therefore calls for a shared vision and should be viewed and addressed in a broader context [ 54 ]. Therefore special attention needs to be given to policies aimed at reducing malnutrition based on the magnitude and nature of determinants of malnutrition, such as poverty, education, health care and family planning services and regional characteristics. Currently in Ghana, various interventions are being implemented to reduce both PEM and micro nutrient deficiencies. These include the Infant and Young Child Feeding Strategy (IYCF) and Community Based Nutrition and Food Security project among others. Notwithstanding the positive effects of these programs, they address only the symptoms of malnutrition and therefore are most likely not sufficient to have a sustained impact in the long term as they do not deal with a lot of the root causes of malnutrition.
The results also suggest that factors strongly associated with average malnutrition are not necessarily also contributing to socioeconomic inequality in malnutrition. The distinction between these groups of variables can be quite important, as it suggests that policies trying to reduce average malnutrition rates can be different from those aiming at lowering socioeconomic inequality in malnutrition. If equity goals are to be achieved, health policies in Ghana should further be directed at strategies/interventions to reduce poverty and to improve the use of health care and family planning services among the poorer population groups. Furthermore, regional disparities should further be tackled to narrow the gap in malnutrition between the poor and the rich. A starting point could be for policy makers to include under-five malnutrition differentials to set criteria to guide resource allocation to regions. Moreover, the strong regional contributions to socioeconomic inequality, even after controlling for other factors such as household wealth and education, bring forward the issue of geographical targeting. Further targeting public programs towards the central and northern regions would substantially reduce socioeconomic inequality in malnutrition and is administratively easier than targeting the poor. The latter argument is relevant for Ghana, where pro-poor policies (redistribution schemes and exemption policies) are not having the aimed effect because of problems in identifying the poor [ 55 , 56 ]. Geographic targeting reduces leakage of program benefits to the non-needy compared to untargeted programs, although under coverage of the truly needy can increase. "Fine-tuning" the targeting by basing it on smaller geographic units increases efficiency, but in some circumstances may be costly and politically unacceptable [ 57 ].
With respect to Ghana, regional averages should be interpreted with caution as there is large heterogeneity between districts in each region and indeed among socio-economic groups within districts. In this case, polices aimed at reducing child malnutrition based on regional averages may lead to under coverage of those in need. [ 58 ] exposes some important limitations of geographic targeting if used to place poverty-alleviation or nutrition interventions within cities. Using data from Abidjan (Cote d'Ivoire) and Accra (Ghana), they found significant clustering in housing conditions; however they did not find any sign of geographic clustering of nutritional status in either city. This implies that geographic targeting of nutrition interventions in these and similar cities has important limitations. Geographic targeting would probably lead to a significant under coverage of the truly needy and, unless accompanied by additional targeting mechanisms, would also result in significant leakage to non-needy populations. Nonetheless, there is a need for additional research to further decompose regional malnutrition inequalities to generate valuable information for policy making decisions. The Ghana Growth and Poverty Reduction Strategy for 2006 – 2009 [ 59 ] states that one of the strategies to be implemented is developing and implementing high impact yielding strategies for malnutrition. This would mean targeting areas at the greatest risks of malnutrition, replicate best practices and expand coverage. This then should result in decreasing malnutrition rates among children particularly in rural areas and northern Ghana.
United Nations Children's Fund (UNICEF): The state of the world's children. 2000, [ http://www.unicef.org/sowc00/ ]
Google Scholar
United Nations (UN): Sub-Saharan Africa – the human costs of the 2015 'business-as-usual' scenario. [ http://hdr.undp.org/docs/events/Berlin/Background_paper.pdf ]
Smith LC, Obeid AEE, Jensen HH: The geography and causes of food insecurity in developing countries. Agricultural Economics. 2000, 22: 199-215. 10.1111/j.1574-0862.2000.tb00018.x.
Article Google Scholar
Smith LC, Haddad L: Explaining child malnutrition in developing countries: a cross country analysis. 2000, International Food Policy Research Institute, Food Consumption and Nutrition Division discussion paper nr. 60
Vella V, Tomkins A, Borghesi A, Migliori GB, Adriko BC, Crevatin E: Determinants of child nutrition in north-west Uganda. Bulletin of the World Health Organization. 1992, 70: 637-647.
CAS PubMed PubMed Central Google Scholar
Pelletier DL, Frongillo EA, Habicht JP: Epidemiological evidence for a potentiating effect of malnutrition on child mortality. American Journal of Public Health. 1993, 83: 1130-1133.
Article CAS PubMed PubMed Central Google Scholar
Schroeder DG, Brown KH: Nutritional status as a predictor of child survival: summarizing the association and quantifying its global impact. Bulletin of the World Health Organization. 1994, 72: 569-579.
Pelletier DL, Frongillo EA: The effects of malnutrition on child mortality in developing countries. Bulletin of the World Health Organization. 1995, 73: 443-448.
Mendez MA, Adair LS: Severity and timing of stunting in the first two years of life affect performance on cognitive tests in late childhood. Journal of Nutrition. 1999, 129: 1555-1562.
CAS PubMed Google Scholar
Delpeuch F, Traissac P, Martin-Pre Y, Massamba JP, Maire B: Economic crisis and malnutrition: socioeconomic determinants of anthropometric status of preschool children and their mothers in an African urban area. Public Health Nutrition. 2000, 3: 39-47.
Article CAS PubMed Google Scholar
Martorell R, Rivera J, Kaplowitz H, Pollitt E: Long-term consequences of growth retardation during early childhood. Human growth: basic and clinical aspects. Edited by: Hernandez M, Argente J. 1992, Amsterdam: Elsevier Science Publishers, 143-149.
Lavy V, Strauss J, Thomas D, de Vreyer P: Quality of health care, survival and health outcomes in Ghana. Journal of Health Economics. 1996, 15: 333-357. 10.1016/0167-6296(95)00021-6.
de Onis M, Frongillo EA, Blossner M: Is malnutrition declining? An analysis of changes in levels of child malnutrition since 1980. Bulletin of the World Health Organization. 2000, 78: 1222-1233.
United Nations (UN): UN Millennium Project. About the Goals: What they are. 2006, [ http://www.unmillenniumproject.org/goals/ ]
United Nations Development Program (UNDP): Human Development Report. 2005
Nolen LB, Braveman P, Dachs JN, Delgado I, Gakidou E, Moser K, Rolfe L, Vega J, Zarowsky C: Strengthening health information systems to address health equity challenges. Bull World Health Organ. 2005, 83 (8): 597-603.
PubMed PubMed Central Google Scholar
Ghana Statistical Service (GSS), Noguchi Memorial Institute for Medical Research (NMIMR), ORC Macro: . Ghana Demographic and Health Survey 2003. 2004, Calverton, Maryland
ORC Macro: Trends in Demographic, Family Planning, and Health Indicators in Ghana, 1960–2003: Trend Analysis of Demographic and Health Surveys Data. 2005, Calverton, Maryland, USA
Shepherd A, Gyimah-Boadi E, Gariba S, Plagerson S, Wahab Musa A: Bridging the North South divide in Ghana. World Development Report 2006, Background Papers. 2004
Ghana Health Service: Imagine Ghana free of malnutrition. Ghana. 2005
Ghana Ministry of Health: National Health Policy Draft. Ghana. 2006
Brakohiapa LA, Yartey J, Bille A, Harrison E, Quansah E, Armar MA, Kishi K, Yamamato S: Does prolonged breastfeeding adversely affect a child's nutritional status?. Lancet. 1988, 332: 416-418. 10.1016/S0140-6736(88)90411-4.
Alderman H: Nutritional status in Ghana and its determinants. Social Dimensions of Adjustments in sub-Saharan Africa. World Bank Working Paper nr 3. 1999, World Bank, Washington
Ruel MT, Levin CE, Armar-Klemesu D, Maxwell D, Morris S: Good care practices can mitigate the negative effects of poverty and low maternal schooling on children's nutritional status: Evidence from Accra. World Development. 1999, 27: 1993-2009. 10.1016/S0305-750X(99)00097-2.
Tharakan CT, Suchindran CM: Determinants of child malnutrition – An intervention model for Botswana. Nutritional Research. 1999, 19: 843-860. 10.1016/S0271-5317(99)00045-7.
Article CAS Google Scholar
Ukuwuani FA, Suchindran CM: Implications of women's work for child nutritional status in sub-Saharan Africa: a case study of Nigeria. Social Science and Medicine. 2003, 56: 2109-2121. 10.1016/S0277-9536(02)00205-8.
Wagstaff A, Watanabe N: Socioeconomic inequalities in Child Malnutrition in the Developing World. World Bank, Policy Research Working Paper 2434;. 2000
Thang NM, Popkin BM: In an area of economic growth, is inequity holding back reductions in child malnutrition in Vietnam?. Asia Pacific Journal of Clinical Nutrition. 2003, 12: 405-10.
PubMed Google Scholar
Zere E, McIntyre D: Inequities in under-five child malnutrition in South-Africa. International Journal for Equity in Health. 2003, 2:
Fotso JC, Kuate-Defo B: Measuring socioeconomic status in health research in developing countries: should we be focusing on households, communities or both?. Social Indicators Research. 2005, 72: 189-237. 10.1007/s11205-004-5579-8.
Hong R: Effect of economic inequality on chronic childhood undernutrition in Ghana. Public Health Nutrition. 2006, 10: 371-378. 10.1017/S1368980007226035.
Wagstaff A, van Doorslaer E, Watanabe N: On decomposing the causes of health sector inequalities with an application to malnutrition inequalities in Vietnam. Journal of Econometrics. 2003, 112: 207-223. 10.1016/S0304-4076(02)00161-6.
World Health Organization Multicentre Growth Reference Study Group: WHO Child Growth Standards: Length/height-for-age, Weight-forage, Weight-for-length, Weight-for-height and Body mass index-for-age: Methods and Development. World Health Organization. 2006, Geneva
Garza C, de Onis M: Rationale for developing a new international growth reference. Food Nutr Bull. 2004, 25 (1 Suppl): S5-S14.
Article PubMed Google Scholar
World Health Organization (WHO): Physical Status: The Use and Interpretation of Anthropometry. WHO Technical Report Series No. 854. 1995, World Health Organization, Geneva
Pradhan M, Sahn DE, Younger SD: Decomposing world health inequality. Journal of Health Economics. 2003, 22: 271-293. 10.1016/S0167-6296(02)00123-6.
World Health Organization: WHO Anthro software and macros. [ http://www.who.int/childgrowth/software/en/ ]
Wagstaff A, Paci P, van Doorslaer E: On the measurement of inequalities in health. Social Science and Medicine. 1991, 33: 545-7. 10.1016/0277-9536(91)90212-U.
Wagstaff A: The Bounds of the Concentration Index When the Variable of Interest is Binary, with an Application to Immunization Inequality. Health Economics. 2005, 14: 429-432. 10.1002/hec.953.
Erreygers G: Correcting the concentration index. Research Paper 2006-027. 2006, Department of Economics, Faculty of Applied Economics, University of Antwerp
Van de Poel E, Hosseinpoor A, Speybroeck N, Van Ourti T, Vega J: Socioeconomic inequalities in malnutrition in developing countries. Bulletin of the World Health Organization. 2007, forthcoming
Fotso J-C: Urban-rural differentials in child malnutrition: Trends and socioeconomic correlates in sub-Saharan Africa. Health and Place. 2007, 13: 205-223. 10.1016/j.healthplace.2006.01.004.
Wooldridge JM: Econometric analysis of Cross Section and Panel Data. 2002, Cambridge, MIT Press
Houweling TAJ, Kunst AE, Mackenbach JP: Measuring health inequality among children in developing countries: does the choice of the indicator of economic status matter?. International Journal for Equity in Health. 2003, 2:
Larrea C, Kawachi I: Does economic inequality affect child malnutrition? The case of Ecuador. Social Science and Medicine. 2005, 60: 165-178. 10.1016/j.socscimed.2004.04.024.
Smith LC, Ruel MT, Ndiaye A: Why is child malnutrition lower in urban than in rural areas? Evidence from 36 developing countries. World Development. 2005, 33: 1285-1305. 10.1016/j.worlddev.2005.03.002.
de Onis M, Onyango A, Borghi E, Garza C, Yang H, for the WHO Multicentre Growth Reference Study Group: Comparison of the World Health Organization child growth standards and the National Center for Health Statistics/WHO international growth reference: implications for child health programmes. Public Health Nutrition. 2006, 9: 942-947. 10.1017/PHN20062005.
Heaton T, Forste R, Hoffmann J, Flake D: Cross-national variation in family influences on child health. Social Science and Medicine. 2005, 60: 97-108. 10.1016/j.socscimed.2004.04.029.
Caldwell J: Education as a factor in mortality decline: An examination of Nigerian data. Population Studies. 1979, 33: 395-413. 10.2307/2173888.
Lindstrom DP, Munoz-Franco E: Migration and maternal health services utilization in rural Guatemala. Social Science and Medicine. 2006, 63: 706-721. 10.1016/j.socscimed.2006.02.007.
Ghana Growth and Poverty Reduction Strategy Paper I (GPRSI): Ghana Poverty Reduction Strategy 2003–2005: An Agenda for Growth and Prosperity. 2003, [ http://siteresources.worldbank.org/GHANAEXTN/Resources/Ghana_PRSP.pdf ]
Ghana Health Service: Facts and Figures 2005. Ghana. 2005, [ http://www.who.int/healthmetrics/tools/logbook/en/countries/gha/2006_Ghana_Fact_and_Figures_Health_2000-05.pdf ]
Wagstaff A, Watanabe N: What difference does the choice of SES make in health inequality measurement?. Health Economics. 2003, 12: 885-90. 10.1002/hec.805.
World Bank: Improving, Health, nutrition and population outcomes in Sub-Saharan Africa. 2004, World Bank, Washington
Chapter Google Scholar
Bosu WK, Nsowah-Nuamah N, Ward PM: A Profile of Health Inequalities in Ghana. Ministry of Health, Ghana. 2000
Bosu WK, Larya-Adjei GL, McIntyre D: A Review of the Ghana Health sector's Pro-poor Agenda. Ghana. 2004
Baker J, Grosh M: Poverty reduction through geographic targeting: How well does it work?. World Development. 1994, 22: 983-995. 10.1016/0305-750X(94)90143-0.
Morris S, Levin CE, Armar-Klemesu M, Maxwell D, Ruel MT: Does geographic targeting of nutrition interventions make sense in cities? Evidence from Abidjan and Accra. World Development. 1999, 27: 2011-2019. 10.1016/S0305-750X(99)00098-4.
Ghana Growth and Poverty Reduction Strategy Paper II (GPRSII): National Development Planning Commission, Ghana. 2005
Filmer D, Pritchett L: Estimating wealth effects without expenditure data – or tears: An application to educational enrolments in states of India. Demography. 2001, 38: 115-132.
Download references
Acknowledgements
Many thanks to Tom Van Ourti, Owen O'Donnell, Eddy van Doorslaer and participants at the UNU-WIDER conference on Advancing Health Equity for useful comments. Ellen Van de Poel acknowledges the University of Antwerp and the World Health Organization for support and funding.
Author information
Authors and affiliations.
Department of Applied Economics, Erasmus University Rotterdam, Burg. Oudlaan 50, 3000 DR Rotterdam, The Netherlands
Ellen Van de Poel
The Faculty of Economics and Commerce, The University of Melbourne, 3010, Victoria, Australia
Equity, Poverty and Social Determinants of Health, Evidence and Information for Policy, World Health Organization, Avenue Appia 20, CH - 1211 Geneva 27, Switzerland
Ahmad Reza Hosseinpoor & Jeanette Vega
Policy Planning Monitoring and Evaluation Division, Ghana Health Service, Private Mail Bag, Ministries, Accra, Ghana
Caroline Jehu-Appiah
Institute of Tropical Medicine, Nationalestraat 155, 2000, Antwerp, Belgium
Niko Speybroeck
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Ellen Van de Poel .
Additional information
Authors' contributions.
EVDP was responsible for the study design, analysis, interpretation of the data and writing of the paper. ARH and NS contributed to formulating the study design, interpreting the data and revising the manuscript. CJA contributed to the writing of the paper and revising the manuscript. JV provided guidance to the work and commented on the manuscript. All authors approved the final version of the paper.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Authors’ original file for figure 1
Authors’ original file for figure 2, authors’ original file for figure 3, rights and permissions.
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License ( http://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Reprints and permissions
About this article
Cite this article.
Van de Poel, E., Hosseinpoor, A.R., Jehu-Appiah, C. et al. Malnutrition and the disproportional burden on the poor: the case of Ghana. Int J Equity Health 6 , 21 (2007). https://doi.org/10.1186/1475-9276-6-21
Download citation
Received : 21 August 2007
Accepted : 28 November 2007
Published : 28 November 2007
DOI : https://doi.org/10.1186/1475-9276-6-21
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Concentration Index
- Birth Interval
- Socioeconomic Inequality
- Family Planning Service
- Demographic Health Survey
International Journal for Equity in Health
ISSN: 1475-9276
- General enquiries: [email protected]
Click through the PLOS taxonomy to find articles in your field.
For more information about PLOS Subject Areas, click here .
Loading metrics
Open Access
Peer-reviewed
Research Article
The epidemiology of undernutrition and its determinants in children under five years in Ghana
Roles Conceptualization, Formal analysis, Methodology, Writing – original draft
* E-mail: [email protected]
Current address: Chinese Center for Endemic Disease Control and Prevention, Harbin Medical University, Harbin, China
Affiliation Ghana Health Service, Bolgatanga, Upper East Region, Ghana
Roles Methodology, Writing – review & editing
Affiliation Department of Family and Consumer Sciences, Faculty of Agriculture, University for Development Studies, Tamale, Ghana
Roles Conceptualization, Writing – review & editing
Affiliation Department of Social Medicine and Health Service Management, Harbin Medical University, Harbin, China
Roles Conceptualization, Writing – original draft
- Michael Boah,
- Fusta Azupogo,
- Daniel Adjei Amporfro,
- Linda Anutua Abada
- Published: July 31, 2019
- https://doi.org/10.1371/journal.pone.0219665
- Reader Comments
Understanding the burden and contextual risk factors is critical for developing appropriate interventions to control undernutrition.
This study used data from the 2014 Ghana Demographic and Health Survey to estimate the prevalence of underweight, stunting, and wasting. Single multiple logistic regressions were used to identify the factors associated with underweight, wasting and stunting. The study involved 2720 children aged 0–59 months old and mother pairs. All analyses were done in STATA/IC version 15.0. Statistical significance was set at p<0.05.
The prevalence of underweight, wasting and stunting were 10.4%, 5.3%, and 18.4% respectively. The age of the child was associated with underweight, wasting and stunting, whereas the sex was associated with wasting and stunting. Normal or overweight/obese maternal body mass index category, high woman’s autonomy and middle-class wealth index were associated with a lower odds of undernutrition. The factors that were associated with a higher odds of child undernutrition included: low birth weight (<2.5 kg), minimum dietary diversity score (MDDS), a higher (≥4 th ) birth order number of child, primary educational level of husband/partner and domicile in the northern region of Ghana.
There is still a high burden of child undernutrition in Ghana. The age, sex, birth weight, birth order and the MDDS of the child were the immediate factors associated with child undernutrition. The intermediate factors that were associated with child undernutrition were mainly maternal related factors and included maternal nutritional status and autonomy. Distal level factors which were associated with a higher odds of child undernutrition were the wealth index of the household, paternal educational status and region of residence. We recommend that interventions and policies for undernutrition should address socioeconomic inequalities at the community level while factoring in women empowerment programmes.
Citation: Boah M, Azupogo F, Amporfro DA, Abada LA (2019) The epidemiology of undernutrition and its determinants in children under five years in Ghana. PLoS ONE 14(7): e0219665. https://doi.org/10.1371/journal.pone.0219665
Editor: Yacob Zereyesus, Kansas State University, UNITED STATES
Received: August 15, 2018; Accepted: June 28, 2019; Published: July 31, 2019
Copyright: © 2019 Boah et al. This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: The dataset for this study is publicly available at www.dhsprogram.com/data/available-datasets.cfm . Interested researchers can replicate our study findings in their entirety by directly obtaining the data from the DHS Program and following the protocol in our Methods section. We did not have any special access privileges that others would not have. Also, the women’s questionnaire is attached to the 2014 GDHS final report downloadable at dhsprogram.com/pubs/pdf/FR307/FR307.pdf .
Funding: The authors received no specific funding for this work.
Competing interests: The authors have declared that no competing interests exist.
Introduction
Malnutrition is a major cause of death among children under five years of age. An estimated 13.6 million children die annually from undernutrition globally [ 1 ]. Mortality in children from undernutrition is highest in developing countries [ 2 ]. At the global level, an estimated 151 million (22.2%) children under-five years of age were stunted in 2016 [ 3 ]. An additional 51 million (7.5%) were at risk of wasting in the same year. Stunting and wasting rates in Africa are above global estimates, albeit inter-country variations. In 2016, stunting affected an estimated 39% of children under-five years while wasting threatened the lives of an estimated 27% [ 4 ].
The causes of malnutrition are multifaceted and include diseases, inadequate diet, environmental, and socioeconomic factors [ 5 ]. The age of the child, gender, birth weight, child’s vaccination status, birth spacing, birth order, maternal education, mother’s body mass index (BMI), antenatal care (ANC) use by mother, household wealth index, improved water, hygiene and sanitation, family structure, and family size have been identified as some of the determinants of children’s nutritional status in sub-Saharan Africa [ 6 – 11 ].
The consequences of poor nutrition during infancy and childhood have been well documented and include impaired growth, poor cognitive and social development, poor school performance, increased risk of morbidity and mortality and reduced productivity later in life [ 2 , 12 – 14 ]. Stunting is linked to poor environmental conditions and repeated exposure to adverse economic conditions that result from poor nutrition during pregnancy and early childhood [ 15 ]. Wasting is a life-threatening result of insufficient food intake and/or disease; it is a measure of acute malnutrition [ 16 ]. Nevertheless, the nutritional status of children can serve as an indicator for measuring the health and well-being of populations; because early childhood health indicators are sensitive to food security situations, environmental, economic and policy changes [ 17 – 19 ]. Thus, they reflect the living conditions to which the child is “exposed” to.
The 2014 Ghana Demographic and Health Survey (GDHS) report shows a decline in neonatal, infant and young child mortality over the past two decades; similarly, malnutrition rates have declined over the same period but remain alarming [ 20 ]. Underweight is falling too slowly while stunting and wasting still impact on the lives of many more children under-five years of age. As a result, both small and large-scale studies have assessed the determinants of childhood undernutrition in Ghana [ 21 – 25 ]. However, these studies are either not generalizable to other parts of the country due to their small sample sizes and location of study [ 24 , 25 ], or they focused on one aspect of undernutrition [ 21 – 23 ].
This study sought to estimate the prevalence of underweight, wasting and stunting, and explore their determinants among children under five years old in Ghana while recognizing the complex hierarchical relationship of these determinants. The findings would be useful in the formulation of policies in Ghana to tackle undernutrition and contribute to the literature by providing evidence on the determinants of the commonly used nutrition profiles for defining undernutrition in children under five at the national level [ 15 , 19 ].
Conceptual framework
The conceptual framework for this study was founded on previous studies that have identified and described risk factors of malnutrition in children [ 5 , 9 , 23 , 26 ]. The framework used is based on the premise that distal factors may determine the nutritional status of children by acting directly or indirectly through some interrelated mediating factors except for age and gender of the child. Briefly, according to our framework, the immediate causes of childhood undernutrition include food, birth weight, the birth order number of the child and diseases. Infections and diarrhoea can decrease food intake and nutrient utilization resulting in poor nutrition, growth, and development of the child [ 27 , 28 ].
Also, the immediate causes of childhood undernutrition are rooted in problems at the household level. Maternal undernutrition during pregnancy can result in low birth weight at birth, which is associated with an increased risk of undernutrition in early childhood [ 29 ]. Large family sizes may lead to inadequate food intake, as do poor access to safe water and sanitation facilities lead to an increase in diseases, which in turn affects food intake and utilization [ 30 ]. Caregivers may seek care for their sick children when health care services are accessible and affordable.
Furthermore, each household level problem, in turn, has its correlated factors at the distal level. As a fact, some household behaviours are modelled by cultural and religious norms prevalent in the community [ 5 ]. Education, employment, household wealth and place of residence are indices of socioeconomic status and may reflect access to resources by the household [ 28 ]. A higher maternal educational level and household wealth index are associated with increased access to household dietary needs, health care services and better living conditions, which are inhibitors of childhood undernutrition [ 31 , 32 ].
Our framework lays out the hierarchical relationship between the risk factors for childhood undernutrition that were examined in this study ( Fig 1 ).
- PPT PowerPoint slide
- PNG larger image
- TIFF original image
https://doi.org/10.1371/journal.pone.0219665.g001
Source of data
We used the child recode dataset of the 2014 GDHS. Approval for the use of the dataset was obtained from ICF international. The Demographic and Health Survey (DHS) is a nationally representative survey that provides coverage data at the population level on key health indicators including reproductive health, fertility, child health, and nutrition from which differences can be assessed by bio-demographic, socioeconomic and geographic characteristics after disaggregation. Details about the survey can be found in the DHS Methodology report [ 33 ].
The 2014 GDHS was carried out by the Ghana Statistical Service (GSS), Ghana Health Services (GHS), and the National Public Health Reference Laboratory (NPHRL) of the GHS. The survey employed a multistage and multi-sampling technique. Sampling units (clusters) were selected in the first stage. The second stage involved the systematic selection of 12, 831 households. Three different questionnaires were used to collect information on household characteristics, fertility, morbidity, mortality and child health. Eligible women for interview were all women aged 15–49 years who were either permanent residents or visitors who stayed in a selected household the night preceding the survey. Weight and height measurements were collected from eligible women and children 0–59 months. Children from selected households were measured irrespective of whether their mothers were interviewed. The sampling frame used was updated from the 2010 population and housing census (PHC). The response rate was 97% for the women’s questionnaire. Height and weight measurements were taken for 3,118 children 0–59 months. However, anthropometric information was available for 2,895 children in the dataset. We excluded children who were flagged for z-scores of nutritional status indices (n = 175), which led to the final sample of 2720 (weighted n = 2636) children under five years of age for analysis. Further details on the survey design and data collection process have been explained elsewhere [ 20 ]. Some variables were recategorized to produce enough sample for data analysis.
Dependent variables.
The three dependent variables in this study were underweight, wasting and stunting. Weight-for-age (WAZ), weight-for-height (WHZ) and height-for-age (HAZ) z-scores of less than -2 standard deviations (SD) from the median according to the 2006 child growth standards of the World Health Organization (WHO) were used to define underweight, wasting and stunting respectively [ 34 ].
The z-scores cut-off point was used to construct binary measures of underweight (WAZ < -2SD), wasting (WHZ < -2SD) and stunting (HAZ < -2SD). A dummy variable with a value of “1” was used in each case to identify children who were underweight, wasted or stunted and “0” for children who are not underweight, wasted or stunted.
Independent variables.
Control variables: the age (in months) and sex of the child were considered as control variables. Age was categorized as 0–5; 6–11; 12–23; 24–35; and 36+ months of age.
The immediate factors (child level factors) included in the study were child’s birth weight; child’s birth order number among other living children; dietary diversity score (DDS); fever and cough episode in the last two weeks before the survey; and diarrhoea episode in last two weeks before the survey. Fever, cough and diarrhoea were considered measures for child’s health status. A DDS comprising 7 food groups was created for the children based on the available data. The food groups included grains, roots and tubers; legumes and nuts; dairy products (cheese, milk, and yoghurt); flesh foods (meat, fish, poultry); eggs; vitamin A rich fruits and vegetables; and other fruits and vegetables [ 35 ]. In the DDS, a score of ‘1’ else ‘0’ was assigned if the child consumed at least one food item from each of the food groups. The aggregated scores of the 7 food groups comprised the DDS which ranged from 0–7. The acceptable minimum DDS was the consumption of foods from at least four food groups.
The intermediate factors (household and maternal factors) included in the study were mother’s age; mother’s parity; mother’s Body-Mass-Index (BMI) categorized as thin (BMI< 18.5kg/m 2 ), normal (BMI 18.5–24.9 kg/m 2 ) and overweight/obese (BMI ≥25 kg/m 2 ); the timing of the first ANC visit; the place used for delivery by the mother; health insurance coverage; woman’s autonomy; household size; type of toilet facility; and source of drinking water. Antenatal care use in Ghana is almost universal [ 20 ]; hence, the timing of the first ANC visit and the place of delivery were used as measures of mother’s health-seeking behaviour during pregnancy and for childbirth. The woman’s autonomy was measured by her involvement in household decision making, attitude towards wife beating and property ownership. A cumulative autonomy index score was created from the summation of individual scores (see supporting material S1 Table ). Tertiles of woman’s autonomy was constructed from the final autonomy index score to provide a measure for woman’s autonomy. This method has been used in other studies [ 36 – 38 ]. The categorization of the type of toilet facility and source of drinking water was guided by the World Health Organization & United Nations Children’s Fund definitions [ 39 ]. The definition of improved household toilet facility was adapted to take into consideration the housing system in some parts of Ghana [ 40 – 42 ]. Therefore, the use of ‘Improved household toilet’ in this study defined all households with access to improved toilet facilities, including those shared with other household members.
The distal factors (socioeconomic and cultural factors) considered were the administrative region, place of residence (rural or urban), mother’s educational level, husband/partner’s educational level, mother’s employment status, household wealth index and religion of the mother. Mother and husband/partner’s educational level was measured by three dummy variables; no formal education, primary, and secondary or higher. The wealth index is a composite measure of a household's cumulative living standard and was calculated in the GDHS by using easy-to-collect data on a household’s ownership of selected assets, such as televisions and bicycles; materials used for housing construction; and types of water access and sanitation facilities. Household wealth quintiles ranging from the poorest to the richest were used as a measure of the wealth index.
Data analysis
It was presumed that the independent variables would exhibit different patterns of relationship across and within hierarchical levels of each of the dependent variables. Therefore, multiple single logistic regressions were preferred over multivariate regression models in identifying the determinants of underweight, wasting and stunting [ 43 ]. Besides, the “svy” command prefix used to adjust for the survey design used by the DHS program can be used with single logistic regression models and not multivariate regression models to produce robust coefficients, standard errors and confidence intervals that are representative. The model fitting process in this study involved three stages.
Firstly, the independent association of each of the distal factors with each of the forms of undernutrition in the absence of the intermediate and immediate factors was assessed (model 1). Secondly, distal factors were fitted with the intermediate factors to assess the association between the intermediate factors and undernutrition adjusting for the confounding effects of distal factors (model 2). Finally, the distal factors and intermediate factors were fitted with immediate factors; this produced the “best fit” independent association between the immediate factors and undernutrition while adjusting for the confounding effects of the distal and intermediate factors and the independent relationship between distal factors and undernutrition (model 3). The age and sex of the child were considered as control variables and maintained in each of the models. The model fitting process was guided by Victora, Huttly, Fuchs, & Olinto [ 44 ].
To avoid an excessive number of parameters and unstable estimates in subsequent models, only variables with a p-value <0.1 were retained in subsequent models [ 45 ]. We entered pairwise interaction terms in order to explore potential nonlinearities, but none of these interactions was statistically significant in the final models. Prevalence estimates with their corresponding confidence intervals (CI) were calculated for the dependent variables, and the Chi-square (χ 2 ) test was used to assess significant differences between the groups. Adjusted odds ratios (AOR) with their corresponding 95% CIs were reported for risk factors. All data analyses were done using STATA/IC version 15.0 for Windows (StataCorp LLC, College Station, Texas USA). The ‘svyset’ and ‘svy’ command prefix, as well as weights, were used to adjust for the complex study design used by the DHS program.
This study did not need any ethical clearance because it is a secondary analysis of data from the 2014 GDHS. The dataset used for the analyses did not contain personal identifiers to respondents or households; the DHS Program protects the privacy of respondents and household members in the surveys. The DHS survey procedures were approved by the Institutional Review Board of ICF Macro International (Calverton, Maryland USA) and the Ethics Review Committee of the Ghana Health Services. Information on the ethical considerations of the DHS survey can be obtained online ( www.dhsprogram.com ). Nonetheless, permission was obtained from ICF to use the dataset. Moreover, the dataset was used for the sole purpose of this study and the sources from which relevant ideas were obtained for this study have been duly referenced.
Sociodemographic characteristics of study participants
The ages of the children ranged from 0–59 months with a mean age of 28.36 ±17.10 months. Of the total children, 11.38% were less than 6 months old. The majority of children were males (52.12%), resident in rural settings (60.84%), from households with 5–9 members (57.59%), households with access to improved toilet facilities (58.22%) and improved drinking water sources (70.54%). About 33% of the children lived in the poorest households. The mean age of the mothers was 30.65±6.89 years. The majority of mothers delivered the index child in a health facility (67.94%), and 69.80% were registered unto the National Health Insurance Scheme (NHIS) ( Table 1 ).
https://doi.org/10.1371/journal.pone.0219665.t001
Prevalence and distribution of underweight, wasting and stunting in children under five years in Ghana by age and sex
From Table 2 , the prevalence of underweight, wasting and stunting was 10.43% [95% CI: 9.10–11.93], 5.31% [95% CI: 4.34–6.48] and 18.37% [95% CI: 16.60–20.28] respectively. There were significant differences between groups for all the three forms of undernutrition by child’s age category. The highest prevalence of underweight (12.81%), wasting (11.44%) and stunting (28.60%) was found among children aged 12–23, 6–11 and 24–35 months, respectively (p<0.05). Female children (16.44%) were less prone to stunting than their male counterparts (20.15%) (p = 0.033).
https://doi.org/10.1371/journal.pone.0219665.t002
Determinants of underweight, wasting and stunting in children under five years in Ghana
Determinants of underweight among children under five years in ghana..
Child’s age, birthweight and mother’s BMI category were significant determinants of underweight after controlling for confounding by the other factors. Underweight was more prevalent among children aged 12–23 months (AOR = 10.65, 95% CI: 1.79–63.32) and 24–35 months (AOR = 11.05, 95% CI: 1.89–64.69) compared to children aged 0–5 months. Relatively, low weight at birth was associated with a higher odds of underweight (AOR = 4.41, 95% CI: 2.17–8.97). Women in the normal and overweight BMI categories were less likely to have underweight children (AOR = 0.36, 95% CI: 0.14–0.92 and AOR = 0.29, 95% CI: 0.10–0.84, respectively) ( Table 3 ).
https://doi.org/10.1371/journal.pone.0219665.t003
Determinants of wasting among children under five years in Ghana.
The determinants of wasting among children under five years have been presented in Table 4 . In the final model, child’s age, sex, dietary diversity score, husband/partner’s educational level, and wealth index were found to be significantly associated with wasting. Comparatively, wasting was less prevalent among children in the age groups of 24–35 months (AOR = 0.24, 95% CI: 0.07–0.79) and 36 months and over (AOR = 0.09, 95% CI: 0.02–0.43). Also, children from the middle-class of the household wealth index were less likely to be wasted (AOR = 0.31, 95% CI: 0.10–0.97). However, female sex (AOR = 2.52, 95% CI: 1.18–5.41), minimum DDS (AOR = 2.46, 95% CI: 1.12–5.39), fourth birth order number of child (AOR = 3.29, 95% CI:1.01–10.71), primary level husband/partner education (AOR = 4.12, 95% CI: 1.39–12.21) were associated with a higher odds of wasting.
https://doi.org/10.1371/journal.pone.0219665.t004
Determinants of stunting among children under five years in Ghana.
Independently, child’s age, birth weight, the birth order of the child, woman’s autonomy and region were identified as determinants of stunting. Stunting was more prevalent among children aged 12–23 months (AOR = 4.54, 95% CI: 1.40–14.74), 24-35months (AOR = 9.99, 95% CI: 3.30–30.24) and 36 months and over (AOR = 5.13, 95% CI: 1.67–15.80). Relatively, children born low birth weight were 3 times more likely to be stunted (AOR = 3.18, 95% CI: 1.70–5.92). Also, birth order of 5 or more was associated with 2 times the odds of stunting (AOR = 2.03, 95% CI: 1.04–3.96). A high woman’s autonomy was associated with a lower odds stunting (AOR = 0.52, 95% CI: 0.28–0.97) whereas children from the northern region of Ghana were about 3 times (AOR = 2.99, 95% CI: 1.13–7.94) more likely to be stunted ( Table 5 ).
https://doi.org/10.1371/journal.pone.0219665.t005
Robustness checks of results
The robustness of our results was ensured and checked. The “svy” command prefix was used in all analyses to adjust for the study design used by the DHS program. The Taylor series linearization method was used to estimate confidence intervals. Survey logistic regressions were used to identify the determinants of undernutrition to account for the study design. The fit of our final models was assessed using the “svylogitgof” which is used for the estimation of the goodness of fit after survey estimations [ 46 ]. We found no evidence of lack of fit of any of our final models as the P -values produced were greater than 0.05.
This study sought to estimate the prevalence of underweight, wasting and stunting among children under five years and identify the determinants of undernutrition in Ghana. The findings showed that the prevalence of underweight, wasting and stunting was 10.4%, 5.3%, and 18.4% respectively. These rates of undernutrition are lower than the rates reported from other countries in Africa, such as Niger, Burundi, Ethiopia, and Mozambique [ 47 , 48 ]. Over the past decade, the Government of Ghana and the Ministry of Health (MoH) have taken concentrate steps in improving maternal, child health and nutrition through the implementation of free antenatal care services, iron and folate supplementation for pregnant women and school feeding activities. These strategies may have contributed to the reduction in the prevalence of undernutrition in children under five years in Ghana. Comparatively, food crises, limited access to arable land for agriculture purposes and adverse climatic conditions have constrained progress in tackling undernutrition in Niger, Burundi, Ethiopia and Mozambique [ 47 , 49 ]; accounting partly for the differences in the prevalence rates of undernutrition between Ghana and the other countries.
The findings also revealed that a child’s age is a determinant of underweight, wasting and stunting. Whereas, the sex is a determinant of wasting and stunting. The risk of underweight increased from the age of 6 months and may be related to the fact that most children in Ghana are breastfed in early life until at 6 months when they transition from only breastfeeding to feeding family foods in addition to breastfeeding which in most cases is characterized by challenges [ 50 , 51 ]. Furthermore, as the age increased from 24 months, the risk of wasting is reduced. On the other hand, stunting expressed itself in children after 11 months but peaked around 24–35 months old. Relatively, male children were more likely to be stunted before the age of 3 years. However, female children were more likely to be wasted than their male counterparts. These findings have been corroborated by other studies [ 19 , 31 , 32 , 51 , 52 ]. The high levels of stunting after 11 months may be explained by repeated exposure to nutritional insults from the prenatal period (first 1000 days).
Nevertheless, the positive association between male sex and stunting has remained controversial. A meta-analysis on gender and stunting concluded that boys in sub-Saharan Africa were more likely to be stunted in early childhood than girls [ 53 ]; this could be due to differences in behaviours, gender inequalities and the biological susceptibility of males to morbidity in early infancy [ 54 ]. However, wasting results from inadequate intake of quality food, and it has been reported elsewhere that in food insecure households, undernutrition is more likely to show in female children relative to males [ 55 ].
At the immediate level, low birth weight was associated with an increased risk of underweight and stunting, which supports findings from a study in Botswana [ 6 ]. A child born low birth weight has already suffered from intrauterine growth retardations and is undernourished at the time of birth [ 55 ]. This undernourished infant may live to be undernourished in early childhood even in the presence of favourable conditions as these conditions may not be sufficient enough to fully compensate for the initial damage caused to the child at birth [ 29 ]. Surprisingly, children who met the minimum DDS were more likely to be wasted compared to their counterparts. This finding contradicts earlier studies in Ghana that reported an inverse relationship between adherence to the minimum DDS and undernutrition [ 27 , 56 ]. The DDS assesses the quality of the child’s food and was assessed with a qualitative 24-hour dietary recall in the DHS. Based on this, the results may not necessarily reflect the usual dietary pattern of the child. Additionally, the DDS was liable to changes in household living conditions as well as the effects of seasonality on food. It is established that seasonal variations can affect the availability and access to especially vitamin A and C-rich foods and in turn, affect the quality and quantity of food consumed by households [ 57 ]. More importantly, the design of the study was cross-sectional, and it may be that undernourished children received extra care in the quality of their food thus, explaining the inverse association between MDDS and undernutrition in this study.
Women are often regarded as primary caregivers; therefore, high woman’s autonomy defined by her freedom to take independent decisions, participate in key decision-making processes and have more control over household resources can impact significantly on decision making with regards to her nutrition and the nutrition of the children [ 47 , 58 ]. This explains the positive association between high autonomy and reduced odds of childhood undernutrition in this study. Also, we found a negative association between maternal BMI category and child underweight. Maternal BMI influences the child’s nutritional status, pre-and-post pregnancy period. During pregnancy, the fetus in an undernourished woman (thin BMI category) is predisposed to adverse growth shocks that contribute to intrauterine growth restrictions [ 1 ]. Also, an undernourished woman faces challenges that include difficulty with breastfeeding, reduced mental abilities, and energy levels that can hinder her ability to take proper care of her children [ 59 ]. The association between maternal undernutrition and poor nutritional outcomes has been reported in Rwanda [ 8 ]. This study did not find any significant association between household size and undernutrition. However, a higher birth order number of the child was significantly associated with an increased odds of wasting and stunting; which could be due to adverse conditions either after delivery or during pregnancy that may have resulted from multiple births by the woman.
At the distal level, children from middle-class households were less likely to be stunted whereas primary level paternal education and residing in the northern region of Ghana were associated with an increased risk of wasting and stunting respectively. Undernutrition is a direct representation of poverty. Individuals from poor households are predisposed to poor living conditions that may result in diseases and poor health outcomes [ 32 ]. Comparatively, middle-class households are financially capable, food secured and have better access to health care services, which are precursors for optimal childhood nutritional outcomes [ 59 ]. The association between increased wealth index and low rates of undernutrition has been reported by other studies [ 8 , 10 ]. A husband/partner’s influence on a child’s nutritional status can be mediated through other factors and not directly. A husband with low educational status (less than secondary) may not be gainfully employed, resulting in poor household wealth status, food insecurity, and poor general living conditions. Additionally, males are more involved in child care by providing financial and physical support to the woman and are less involved in decision making regarding appropriate infant and young child feeding practices [ 60 ]. The northern region of Ghana lies in the savannah zone. Hence, the high prevalence of stunting in the region can partly be explained by the ecological constraints, food insecurity and poverty in the region [ 32 , 52 ].
Some strengths and limitations should be taken into account when interpreting the findings of this study. The study participants in the GDHS 2014 were women who delivered in the past five years preceding the survey. The extended period, therefore, subjects some parts of the data such as the timing of the first ANC visits to recall biases except for the anthropometric measurements. The magnitude of the recall bias is unknown and correcting it is impossible. However, it is assumed that the biases are to a moderately sufficient extent random. The DHS survey also employed a cross-sectional study design and therefore, does not depict any causal link. We, therefore, limit our interpretation to describing associations. Nonetheless, we thoroughly modelled several potential explanatory variables including subject and household demographics, education, livelihood and socio-economic conditions, which may be contributing to child nutritional status. Lastly, we employed robust statistical models with weighting factors while accounting for the effects of clustering and stratification in the data.
The aetiology of undernutrition in Ghana is multifaceted and interconnected. The nutritional status of children under five years is determined by socioeconomic, cultural, household, maternal, and child level factors. The effect of socioeconomic factors on underweight, wasting and stunting is exhibited independently and mediated through maternal and child level factors.
It is logical to conclude that empowering women as well as improving the socioeconomic status of households may contribute significantly to reducing morbidity and mortality from undernutrition. We recommend that nutritional interventions to fight childhood undernutrition should take into consideration policies or strategies that would empower women, and address socioeconomic inequalities at the community level.
Supporting information
S1 table. woman’s autonomy score index..
https://doi.org/10.1371/journal.pone.0219665.s001
Acknowledgments
We thank the ICF International for permitting us to use the 2014 GDHS child recode dataset for our study. We acknowledge the support of Isaiah Agorinya during the data analysis.
- View Article
- PubMed/NCBI
- Google Scholar
- 3. United Nations Children’s Fund, World Health Organization, World Bank Group. Levels and trends in child malnutrition: Key findings of the 2018 Edition of the Joint Child Malnutrition Estimates. United Nations Children’s Fund; 2018. www.who.int/nutgrowthdb/estimates
- 4. World Health Organization. Nutrition in the WHO African Region. Brazzaville; 2017. www.afro.who.int
- 13. WHO. Nutrition Landscape Information System (NLIS). Country Profile Indicators. Interpretation Guide. 2010.
- 20. Ghana Statistical Service, Ghana Health Service, ICF International. Ghana Demographic and Health Survey, 2014. Rockville, Maryland, USA; 2015.
- 30. Annette P-Ü, Robert B, Fiona G, Bartram J. Safer water,better health: costs, benefits and sustainability of interventions to protect and promote health. Geneva: World Health Organization; 2008. www.apps.who.int/publications/2008/9789241596435_eng.pdf
- 33. Demographic and Health Survey. Guide to DHS statistics. Demographic and Health Surveys Methodology. Rutstein SO, Rojas G, editors. Calverton, Maryland, Maryland, USA: Demographic and Health Surveys, ORC Macro; 2006.
- 34. World Health Organization. WHO Child Growth Standards. 2006. www.int/childgrowth/standards/technicalreport
- 35. World Health Organization, UNICEF, USAID, AED, UCDAVIS, IFPRI, et al. Indicators for assessing infant and young child feeding practices Part 3: Country Profiles. 2010. pp. 1–58.
- 39. World Health Organization, United Nations Children’s Fund. Progress on drinking water, sanitation and hygiene: 2017 update and SDG baselines. Geneva; 2017. www.wssinfo.org
- 49. Salami A, Kamara AB, Brixiova Z. Smallholder Agriculture in East Africa: Trends, Constraints and Opportunities. Working Paper Series. Tunis, Tunisia, Tunisia; 2010. Report No.: 105.
- 58. Bold M van den, Quisumbing AR, Gillespie S. Women’s Empowerment and Nutrition; An Evidence Review. Washington, DC: International Food Policy Research Institute(IFPRI); 2013.
Measuring the Overall Burden of Early Childhood Malnutrition in Ghana: A Comparison of Estimates From Multiple Data Sources
Affiliations.
- 1 Research Department, Saskatchewan Health Authority, Regina, SK, Canada.
- 2 Department of Sociology, University of Saskatchewan, Saskatoon, SK, Canada.
- 3 School of Epidemiology and Public Health, Faculty of Medicine, University of Ottawa, Ottawa, ON, Canada.
- 4 Faculty of Kinesiology and Health Studies, University of Regina, Regina, SK, Canada.
- 5 Department of Mathematics and Statistics, University of Energy and Natural Resources, Sunyani, Ghana.
- 6 Department of Sociology & Anthropology, Mount Saint Vincent University, Halifax, NS, Canada.
- PMID: 33589568
- PMCID: PMC9808187
- DOI: 10.34172/ijhpm.2020.253
Background: Childhood malnutrition contributes to nearly half (45%) of all deaths among children under 5 globally. The United Nations' Sustainable Development Goals (SDGs) aims to end all forms of malnutrition by 2030; however, measuring progress towards these goals is challenging, particularly in countries with emerging economies where nationally-representative data are limited. The primary objective of this study was to estimate the overall burden of childhood malnutrition in Ghana at national and regional levels using 3 data sources.
Methods: Using data from the long-standing Ghana Demographic and Health Surveys (GDHS), Ghana Multiple Indicator Cluster Survey (GMICS), and the emerging Ghana Socioeconomic Panel Survey (GSPS), we compared the prevalence of malnutrition using the extended composite index of anthropometric failure (eCIAF) for the period 2008- 2011. This study included data for children aged 6-59 months and calculated all anthropometric z-scores based on the World Health Organization (WHO) Growth Standards. We tested for differences in malnutrition subtypes using two-group configural frequency analysis (CFA).
Results: Of the 10 281 children (6532 from GMICS, 2141 from GDHS and 1608 from GSPS) included in the study, the only demographic difference observed was the children included in the GSPS were slightly older than those included in the GDHS and GMICS (median age of 36 vs 30 vs 33 months, P <.001). Based on the eCIAF, the overall prevalence of malnutrition at the national level was higher among children in the GSPS (57.3%, 95% CI: 53.9%-60.6%), followed by the GDHS (39.7%, 95% CI: 37.0%-42.5%), and then those in the GMICS (31.2%, 95% CI: 29.3%-33.1%). The two-group CFA showed that the 3 data sources also estimated different prevalence rates for most of the malnutrition subtypes included in the eCIAF.
Conclusion: Depending on the data source adopted, our estimates of eCIAF showed that between one-third and half of all Ghanaian children aged 6-59 months had at least one form of malnutrition over the period 2008-2011. These eCIAF estimates should complement the commonly reported measures such as stunting and wasting when interpreting the severity of malnutrition in the country to inform policy decisions.
Keywords: Demographic Health Survey; Ghana; Prevalence of Malnutrition; Sustainable Development Goals; Under Nutrition.
© 2022 The Author(s); Published by Kerman University of Medical Sciences This is an open-access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Child, Preschool
- Cross-Sectional Studies
- Ghana / epidemiology
- Information Sources*
- Malnutrition* / epidemiology
- High contrast
- ABOUT UNICEF
- THE CONVENTION ON THE RIGHTS OF THE CHILD
- THE SITUATION OF CHILDREN IN GHANA
- Work for UNICEF
- PRESS CENTRE
Search UNICEF
National nutrition policy, a report on micro-nutrient deficiencies, stunting and the emerging issue of over-nutrition.

Despite appreciable reductions in malnutrition rates significant numbers of people in Ghana, especially women and children are still affected by micro-nutrient deficiencies, stunting and emerging issue of over-nutrition that ultimately undermine their health and development.
Indeed the gains made have not equitable across all areas of the country and across all categories of women and children, with wide geographical and socio-economic disparities. This is largely because interventions have not been implemented at scale in all parts of the country in a sustainable and coordinated manner across relevant sectors.

Files available for download
Related topics, more to explore.
Ghana, Japan, and UNICEF boost the COVID-19 vaccination drive with 30 new ultra-cold chain equipment for storage of vaccines
Making a difference with timely support and investment – Osm
Reducing malnutrition and child deaths through timely actions
A healthy brain and body start from what goes inside
Raising young nutrition champions for healthier generations
Nutrition crisis looms as globally more than 39 billion in-school meals missed since start of COVID-19 pandemic – UNICEF and WFP
Effects of Long-Term Malnutrition on Education Outcomes in Ghana: Evidence from a Panel Study
- Original Article
- Published: 12 January 2021
- Volume 34 , pages 1–21, ( 2022 )
Cite this article

- Robert D. Osei 1 &
- Monica P. Lambon-Quayefio ORCID: orcid.org/0000-0003-4126-6430 2
688 Accesses
2 Citations
3 Altmetric
Explore all metrics
Aside the direct effect on GDP at the macro level, the microeconomic impacts of undernutrition are also manifested in lower educational outcomes, reduced productivity and reduced lifetime earnings. This study sought to examine the effect of child malnutrition on learning outcomes by exploiting a nationally representative panel data which allow us to control for child-level unobserved heterogeneity in Ghana. Using a random-effects and Poisson estimations, this study shows that while current malnutrition affects children’s learning outcomes negatively, its effect may disappear in the future, especially with the implementation of appropriate interventions. The study concludes that while nutrition matters for learning outcomes, so do other educational inputs. Results are, however, differentiated by individual and household characteristics, including gender and locality. The evidence from this study serves as a useful tool for improving policies and programmes that focus on early feeding practices among pre-schoolers and improved nutrition of children of school-going age.
Outre l’effet direct sur le PIB au niveau macro, les impacts microéconomiques de la sous-nutrition se manifestent également par des résultats scolaires moindres, une productivité réduite et des revenues moindres tout au long de la vie. Cette étude visait à examiner l’effet de la malnutrition infantile sur la capacité d’apprentissage en exploitant des données de panel représentatives au niveau national, ce qui nous permet de contrôler la non-hétérogénéité au niveau des enfants au Ghana. En utilisant les estimations du modèle à effets aléatoires et du modèle de Poisson, cette étude montre que si la malnutrition a un effet négatif sur la capacité d’apprentissage des enfants sur le moment, cet effet peut disparaître avec le temps, en particulier grâce à la mise en œuvre d’interventions adaptées. L’étude conclut que si la nutrition est importante pour la capacité d'apprentissage, il en va de même pour les autres facteurs éducatifs. Les résultats sont toutefois différenciés selon les caractéristiques individuelles et celles des ménages, notamment le sexe et la localité. Les données probantes qui émanent de cette étude représentent un outil utile pour l’amélioration des politiques et des programmes qui se concentrent sur les pratiques alimentaires précoces chez les enfants d'âge préscolaire et sur l'amélioration de la nutrition des enfants en âge d'aller à l'école.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
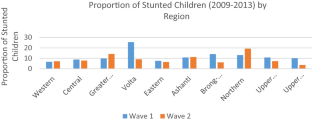
Source based data from Ghana Socio-Economic Panel Survey (2009/2010–2012/2013)
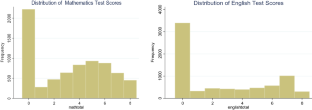
Similar content being viewed by others

The Implication of Early Childhood Malnutrition for Age of Entry into Primary School in Nigeria

Maternal education and child malnutrition: evidence from selected West African countries

Measuring socioeconomic gaps in nutrition and early child development in Bolivia
Agresti, A. 2002. Categorical Data Analysis . New York: Wiley.
Book Google Scholar
Alderman, H. 2006. Long-Term Consequences of Early Childhood Malnutrition. Oxford Economic Papers 58 (3): 450–474.
Article Google Scholar
Alderman, H., J. Behrman, V. Lavy, and R. Menon. 2001. Child Health and School Enrollment. Journal of Human Resources 26 (1): 185–205.
Alderman, H., D. Gilligan, and K. Lehrer. 2012. The Impact of Food for Education Programs on School Participation in Northern Uganda. Economic Development and Cultural Change 61: 187–218.
Alderman, H., J. Hoddinott, and B. Kinsey. 2006. Long-Term Consequences of Early Childhood Malnutrition. Oxford Economic Papers 58: 450–474.
Allison, P. 1999. Logistic Regression Using the SAS System: Theory and Applications . Cary: SAS Institute.
Google Scholar
Ampaabeng, S., and C. Tan. 2013. The Long-Term Cognitive Consequences of Early Childhood Malnutrition: The Case of Famine in Ghana. Journal of Health Economics 32: 1013–1027.
Barron, D. 1992. The Analysis of Cout Data: Over-dispersion and Autocorrelation. In Sociological Methodology , ed. V. Peter. Marsden: Blackwell.
Behrman, J., H. Alderman, and J. Hoddinott. 2004. Hunger and Malnutrition. In Global Crises, Global Solutions , ed. B. Lomborg. Cambridge: Cambridge University Press.
Belachew, T., et al. 2011. Food Insecurity, School Absenteeism and Educational Attainment of Adolescents in Jimma Zone Southwest Ethiopia: A Longitudinal Study. Nutrition Journal 10: 29.
Bull, R., K. Epsy, and S. Wiebe. 2008. Short-Term Memory, Working Memory, and Executive Functioning in Pre-schoolers: Longitudinal Predictors of Mathematical Achievement at Age 7 Years. Developmental Neuropsychology 33 (3): 205–228.
Buttenheim, A., H. Alderman, Friedman, J. 2011. Impact Evaluation of School Feeding Programs in Lao PDR. Policy Research Working Paper Series 5518. The World Bank.
Cameron, A., and P. Trivedi. 1998. Regression Analysis of Count Data . New York: Cambridge University Press.
Daniels, M., and L. Adair. 2004. Growth in Young Filipino Children Predicts Schooling Trajectories Through High School. The Journal of Nutrition 134 (6): 1439–1446.
Feyrer, J., D. Politi, and D. Weil. 2017. The Cognitive Effects of Micronutrient Deficiency: Evidence from Salt Iodization in the United States. Journal of the European Association 15 (2): 355–378.
Ghana Statistical Service. 2012. Ghana multiple indicator cluster survey with an enhanced Malaria module and biomarker 2011. Accra: GSS (Available at http://dhsprogram.com/pubs/pdf/FR262/FR262.pdf ).
Glewwe, P. 2005. The Impact of Child Health and Nutrition on Education in Developing Countries: Theory, Econometric Issues, and Recent Empirical Evidence. Food and Nutrition Bulletin 26 (2_Suppl): S235–S250.
Glewwe, P., and E.A. Miguel. 2008. The impact of child health and nutrition on education in less developed countries. In Handbook of Development Economics , vol. 4, ed. H.B. Chenery, 3561–606. Amsterdam: Elsevier.
Glewwe, P., Jacoby, H., King, E., et al. 2001. Early childhood nutrition and academic achievement: A longitudinal analysis. Journal of Public Economics 81 (3): 345–368.
Grantham-McGregor, S., and L. Fernald. 1999. Effects of Health and Nutrition on Cognitive and Behavioural Development in Children in the First Three Years of Life. Part 1: Small for Gestational Age, Breastfeeding and Protein-Energy Malnutrition. Food Nutrition Bulletin 20: 53–75.
Grantham-McGregor, S., and S. Walker. 1998. Health and Nutritional Determinants of School Failure, Nutrition, Health and Child Development Research Advances and Policy Recommendations . Washington, DC: PAN American Health Organization.
Greve, J., M. Schultz-Nielson, and E. Tekin. 2017. Fetal Malnutrition and Academic Success: Evidence from Muslim Immigrants in Denmark. Economics of Education Review 60: 20–35.
Hoddinott, J., et al. 2013. The Economic Rationale for Investing in Stunting Reduction. Maternal and Child Nutrition 8 (Suppl 2): 69–82.
Horton, S., and J. Ross. 2003. The Economics of Iron Deficiency. Food Policy 28: 51–75.
Kazianga, H., D. de Walque, and H. Alderman. 2009. Educational and Health Impacts of Two School Feeding Schemes: Evidence from a Randomised Trial in Rural Burkina Faso. Policy Research Working Paper Series 4976. The World Bank
Lindsey, J. 1995. Modelling Frequency and Count Data . Oxford: Oxford University Press.
Martins, V., et al. 2011. Long-Lasting Effects of Undernutrition. International Journal of Environmental Research and Public Health 8 (6): 1817–1846.
McCullagh, P., and J. Nelder. 1989. Generalised Linear Models , 2nd ed. London: Chapman and Hall.
National Development Planning Commission. 2016. The cost of hunger in Africa: Social and economic impact of child undernutrition on Ghana’s long term development. Accra: NDPC.
Osberg, L., and K. Xu. 1999. Poverty Intensity: How Well Do Canadian Provinces Compare? Canadian Public Policy XXV (2): 179–195.
Pollit, E. 1990. Malnutrition and infection in the classroom. Summary and Conclusions. Food and Nutrition Bulletin 12: 3.
Prendergast, A., and J. Humphrey. 2014. The Stunting Syndrome in Developing Countries. Paediatrics and International Child Health 34: 250–265.
Ross, A. 2010. Nutrition and Its Effects on Academic Performance. MAE Thesis, Northern Michigan University, Marquette.
Rosso, J., and T. Marek. 1996. Class Action: Improving School Performance in the Developing World Through Better Health and Nutrition . Washington, DC: World Bank.
Schultz-Nielson, M., E. Tekin, and J. Greve. 2016. Labour Markets Effects of Intrauterine Exposure to Nutritional Deficiency: Evidence from Administrative Data on Muslim Immigrants in Denmark. Economics and Human Biology 21: 196–209.
Wechsler, D. 1991. Wechsler Intelligence Scale for Children. Third Edition (WISC-III). San Antonio: The Psychological Corporation.
WHO. 2008. Training Course on Child Growth Assessment . Geneva: World Health Organisation.
Wisniewski, S. 2010. Child Nutrition, Health Problems and School Achievement in Sri Lanka. World Development 38: 315–332.
Yamauchi, F. 2006. Early childhood nutrition, schooling and sibling inequality in a dynamic context: Evidence from South Africa. Discussion paper no. 203, international dood policy research institute, Washington, DC.
Yawson, A., et al. 2017. The Lancet in Ghana: A Determinants Analysis Approach to Inform Strategic Nutrition Planning. BMC Nutrition 3 (1): 27.
Download references
Author information
Authors and affiliations.
Institute of Statistical Social and Economic Research, University of Ghana, Legon, P.O. Box LG 74, Accra, Ghana
Robert D. Osei
Economics Department, University of Ghana, Legon, P.O. Box LG 57, Accra, Ghana
Monica P. Lambon-Quayefio
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Monica P. Lambon-Quayefio .
Ethics declarations
Conflict of interest.
On behalf of the authors, the corresponding author states that there is no conflict of interest.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Reprints and permissions
About this article
Osei, R.D., Lambon-Quayefio, M.P. Effects of Long-Term Malnutrition on Education Outcomes in Ghana: Evidence from a Panel Study. Eur J Dev Res 34 , 1–21 (2022). https://doi.org/10.1057/s41287-020-00350-4
Download citation
Accepted : 04 December 2020
Published : 12 January 2021
Issue Date : February 2022
DOI : https://doi.org/10.1057/s41287-020-00350-4
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Malnutrition
- Learning outcomes
- Random effects
- Cognitive skills
- Find a journal
- Publish with us
- Track your research
- Research article
- Open access
- Published: 15 March 2017
The lancet series nutritional interventions in Ghana: a determinants analysis approach to inform nutrition strategic planning
- A.E. Yawson 1 ,
- E.O. Amoaful 2 ,
- L.K. Senaya 3 ,
- A.O. Yawson 4 ,
- P.K. Aboagye 2 ,
- A.B. Mahama 5 ,
- L. Selenje 5 &
- V. Ngongalah 5
BMC Nutrition volume 3 , Article number: 27 ( 2017 ) Cite this article
10k Accesses
9 Citations
3 Altmetric
Metrics details
Malnutrition is a leading cause of mortality and morbidity among children in low- and middle-income countries. Ghana is one of 36 countries with the highest burden of stunting, globally. The aim of this work is to use data driven planning methods to conduct in-depth analysis on the Lancet series nutrition interventions in Ghana to inform nutritional strategic planning.
A mixed methods approach was employed for this national nutritional assessment conducted in May 2016. Quantitative data on nutritional interventions were generated by application of the Determinants Analysis Tool and phenomenological approach was employed to explain the causes of barriers identified. Outputs from the tool were analyzed by simple descriptive statistics and data from group discussions were assessed by thematic content analysis. The base line years for this assessment were 2014 and 2015.
Overall in Ghana, 21.0% of frontline health workers are trained on lactation management and breastfeeding counselling and support, 56.6% of mothers of children 0–2 years initiated breastfeeding within one hour of birth, and 59.4% of mothers with children 0–5 months took iron folate supplementation for 90 or more days during pregnancy. In addition, only 19.9% of children 12–59 months received two doses of vitamin A supplementation in a calendar year, and 32.5% of children 6–59 months with severe acute malnutrition were admitted for treatment at health facilities. In all, among infants 6–8 months old, 6.9% were fed with minimum dietary diversity, 50.6% received age appropriate meal frequency and 21.6% received iron rich diet. Inadequate pre-service and in-service training for staff, low prioritization and coordination (at higher levels) and weak integration of services (at lower levels) were key barriers to nutrition coverage in Ghana.
Data driven analysis and planning based on proven nutritional interventions in Ghana demonstrated gaps and barriers and garnered workable strategies to improve nutrition services.
Peer Review reports
Malnutrition is a leading cause of mortality and morbidity among children in low- and middle-income countries [ 1 , 2 ]. In Sub-Saharan Africa, under nutrition constitutes a leading cause of death in children under five years old [ 3 , 4 ]. Multiple interventions and multi-sectoral approach are needed to prevent different aspects of nutritional depletion and deprivation such as severe malnutrition, anaemia, wasting and stunting [ 2 , 5 , 6 ].
The implications and consequences of these nutritional deprivation in later adult life make it imperative for national nutritional programmes to focus on sufficient feeding for individuals, families and communities as well as a responsive health care delivery system [ 3 , 7 , 8 ]. Child malnutrition within a household is greatly influenced by issues at national and regional levels [ 9 ].
Ghana is beset with under nutrition among children, and is one of 36 countries with the highest burden of stunting, globally [ 4 ]. In Ghana 19% of children are stunted, 5% of children are wasted and 11% of children are underweight [ 10 ]. Anaemia as a result of under nutrition among children is another key national challenge, 66% of children aged 6–59 months have some level of anaemia, 37% have moderate levels of anaemia and 2% have severe anaemia [ 10 , 11 ]. National coverage on interventions is relatively low with inadequate engagement of the health sector and other sectors to address food security, food safety and hygiene for sustained improvement [ 12 ].
Current national efforts to reduce nutritional deprivations in Ghana include building capacity of service providers and volunteers in nutritional counselling, and improving knowledge and skill of service providers in the management of severe acute malnutrition [ 12 , 13 ]. In addition, national scale up of infant and young child feeding activities include strengthening health care practices through the Baby-Friendly Hospital Initiative and creating demand for services through participation of local leaders and communities on sociocultural practices around malnutrition [ 12 , 13 ].
Progress has been made over the past decade, as demonstrated in the 2014 Demographic and Health Survey (GDHS) [ 10 ]. Infant mortality declined from 77 deaths per 1,000 live births in 1988 to 41 in 2014 and under-5 mortality declined substantially from 155 to 60 death per 1,000 live births over the same period. These improvements at the national level notwithstanding, inequities exist in status of children by regional and geographical location in the country [ 10 , 11 ]. Under-5 mortality in 2014 ranged from 47 deaths per 1,000 live births in Greater Accra (the capital region) to 111 deaths per 1,000 live births in Northern region (a predominantly rural region), while stunting ranged from 10.4% in Greater Accra to 33.1% in the Northern Region. The improvements in anaemia, stunting and wasting among children in Ghana have generally been uneven, with wide geographical disparities and among different wealth quintiles [ 10 ].
Interestingly, the burden of nutrition in Ghana is not limited to children because adult men and women are affected as well. In adults under- and over nutrition are both demonstrated through national surveys to be a health challenge. Overall, among men and women aged 15–49 years, 6% of women and 10% of men are underweight (Body Mass Index, BMI <18.5), while 40% of women and 16% of men are overweight (BMI > =25.0) [ 10 ].
Major causes and determinants of malnutrition in Ghana include, inadequate diet diversity (insufficient food/nutrient intake and inadequate consumption of foods rich in micronutrients and protein including eggs and legumes); poor environmental, household and individual hygiene including hand hygiene practices; as well as generally poor infant and young child feeding practices [ 12 ].
This assessment of national nutrition interventions based on The Lancet Series-Maternal and Child Nutrition [ 14 , 15 ] was thus intended to determine the status of these proven nutritional interventions in Ghana, identify barriers to service provision and develop workable strategies. It used data driven planning methods to conduct in-depth analysis needed to guide programme scale up and targeting, to improve coverage and scope of proven nutritional interventions.
Mixed methods approach were employed for this national nutritional assessment conducted in May 2016. Quantitative data on nutritional interventions was generated by application of the Determinants Analysis Tool and phenomenological approach was employed to explain the causes of barriers identified. Four participants (Regional Deputy Director of Public Health, Regional Public Health Nurse, Regional Nutrition Officer and Regional Health Information Officer) were purposively selected from each of the ten administrative regions in the Ghana due to their background and role in nutrition services. In addition local facilitators (Nutrition Unit of the Ghana Health Service) and representatives from some development partners (including UNICEF, WHO and World Food Programme (WFP) participated. Ghana has ten administrative regions, and officers from all ten regions were included to provide a nationwide representation. The national assessment was undertaken in the Ashanti Region of Ghana for three days to assess barriers to coverage of nutrition services and included desk review, group discussions and key informants interviews. Facilitators assisted in the desk reviews, conduct of interviews and provided mentoring and coaching on capturing major issues and recording of key points from the group discussion.
Main causes of identified bottlenecks to the nutritional interventions were thematically analysed through a phenomenological approach under service delivery factors and enabling environment factors through group discussions. Phenomenological approach was used to allow a deeper understanding of an event or phenomenon by looking at the story of the group who experienced a shared lived experience or phenomenon [ 16 ]. Six teams made up of regional, national and international personnel were formed in line with the key interventions to provide qualitative explanation and assessment of the outputs from the tool.
The determinants analysis framework
The Determinants Analysis framework is premised on the notion that effective coverage of services is influenced by four main factors or determinants namely: supply, demand, quality and environment. The Ten Determinant Model Tool produces a graphical output (Fig. 1 ) that facilitates identification of the key bottlenecks.
Graphical presentation of the determinants analysis framework. Description of figure: The figure describes the supply side, demand side and effective coverage determinants and how bottlenecks are determined
Overall, the Ten Determinant Model used for this nutrition assessment in Ghana had FOUR Domains with TEN Determinants: Enabling Environment (Social Norms, Management/Coordination, Legislation/Policy and Budget/Expenditures); Supply (Commodities, Human Resource and Access); Demand (Initial Utilisation, Continuous Utilisation/Knowledge) and Effective Coverage/Behaviour [ 17 , 18 ].
Identification of the low bars on the supply-determinant side of the graph as well as a sharp drop from one bar to the next on the demand and quality-determinant side of the graph enables managers to identify and prioritize bottlenecks to the effective health service coverage.
Data collection
The Ten Determinant Model is based on Microsoft Excel sheets linked together with sections for data inputs linked to outputs. Input data produce simple bar graphs that display the determinants of health service coverage and thus facilitate identification of key bottlenecks that influence effective coverage (illustrated in Fig. 1 ). The section for data input is fully linked with the section that displays the outputs. The tool directly utilised data from District Health Information Management System (DHIMS), Multi-Indicator Cluster Survey (MICS) Reports [ 19 ], Demographic and Health Surveys (DHS) [ 20 ] and other sources of data including programme monitoring and review reports. The DHIMS is a tool for collection, validation, analysis, and presentation of aggregate statistical data, tailored to integrated health information management activities in the Ghana Health Service.
Outcome measures and data analysis
Six key nutrition tracer interventions based on The Lancet Series-Maternal and Child Nutrition [ 15 ], were selected as, Community Management of Acute Malnutrition (CMAM), Complementary Feeding, Early Initiation to Breastfeeding, Exclusive Breastfeeding, Vitamin A Supplementation, and Iron-Folic Acid Supplementation . Each intervention was assessed based on a particular delivery platform (as individualized facility based services or schedulable and outreach services or as family oriented practices and community based services) to enable accurate identification of barriers and bottlenecks. In this analysis, minimum acceptable diet for complementary feeding was assessed using two sub components-minimum dietary diversity and age appropriate meal frequency as specified in the Ministry of Health National Nutrition Policy of Ghana [ 12 ]. Each of the six thematic groups had a moderator and a recorder. Data from group discussions were organized and described using manual thematic content analysis for qualitative data. Each group worked on a different theme to eliminated the issue of duplication and repetition of information among the groups. Quantitative data were analyzed with simple descriptive statistics (i.e. proportions and percentages) by Microsoft Excel 2013.
The base line years for this assessment were 2014 and 2015 and national coverage targets were used as the benchmark to assess these coverage indicators. Outputs from the tool were analyzed by simple descriptive statistics such as frequency, proportions and ratios. The determinants analysis principles were applied to identify bottlenecks. Causality analysis were conducted to identify barriers resulting in these bottleneck. This formed the basis in determining strategies to remove the bottlenecks on nutritional deprivation in Ghana.
Ethical Issues
All data used was aggregated data at national level and had no link to individuals. In all cases, documentations and computerized records were kept secure and accessible to persons directly involved in developing the operational plans. The Ghana Health Service Ethics Review Committee and office of the Policy, Planning, Monitoring and Evaluation Division of the Ghana Health Service gave approval for documentation and dissemination of the Determinant Analysis process in Ghana.
The assessment provided quantitative values on the performance of each indicator from outputs of the tool, while qualitative explanation and assessment of identified bottlenecks was through causality analysis and group discussions. Details of the analysis are indicated in a comprehensive descriptive Table (Table 1 ).
Maternal and child undernutrition, consisting of stunting, wasting, and deficiencies of essential vitamins and minerals, was the subject of a Series of papers in The Lancet in 2008 [ 4 , 7 , 14 ]. It was suggested then that, long-term consequences of undernutrition could be reduced through high and equitable coverage of proven nutrition interventions. Included in these were the nutrition specific interventions [ 4 , 7 , 14 ]. Lancet series have been in existence close to eight years and have provided guidance to countries in their quest to improve health and nutrition of children under five years of age and Ghana is no exception. Six of the key nutrition specific interventions were selected for assessment at the national level in Ghana.
The analysis readily highlighted gaps in service coverage quantitatively (from service and survey data) and provided a platform for qualitatively analyzing barriers and bottlenecks in the continuum of care for the newborn. These discussions included key service providers and policy makers with sufficient knowledge of the context of nutritional service delivery in Ghana.
The current national efforts to reduce nutritional deprivations in Ghana outlined in the National Nutrition Policy of 2013 include building capacity of service providers and volunteers in nutritional counselling, improving knowledge and skill of service providers in the management of severe acute malnutrition and a national scale up of infant and young child feeding activities by strengthening health care practices through the Baby-Friendly Hospital Initiative [ 12 , 13 ]. In addition, a number of initiatives and frameworks have been developed and implemented by the national Ministry of Health to address the problem of high under five mortality including the Child Health policy, Millennium Accelerated Framework, Accelerated immunization with introduction of new and additional vaccines, as well as the Global Funded programmes for Malaria, Tuberculosis and HIV [ 12 ].
The challenge has been major gaps in access and utilization of these interventions and the reality however is that, most of these interventions and frameworks have been centrally developed with little attention paid to data driven approaches and causal analysis of barriers at the service delivery level.
To overcome these challenges, the current analysis based the national nutritional strategies on the framework developed by Bezanson and Isenman in 2010 [ 21 ] to provide guidance as Ghana implements the national nutrition policy. The ‘Framework for Action for Scaling Up Nutrition’ in 2010 was based on a broad collaborative effort of the World Bank, United Nations Children Fund (UNICEF), World Health Organization (WHO), World Food Programme (WFP) and a wide range of other international partners from developing countries, with the objective to catalyse actions to move undernutrition toward the centre stage of international discourse [ 21 ].
The action oriented framework from a national discourse (key service providers, policy managers and health managers) is aimed to garner local and governmental support to improving stunting, wasting and anaemia, and reduce inequities- in a setting situated among the lowest 32 countries with such health indices [ 4 ].
A summary of the key elements of the framework is provided as a template and shown in Table 2 .
Key lessons learned
Good quality data are essential for effective planning and analysis, and data validation to improve data quality and accuracy is a core activity that should be undertaken by all levels of the health system. The Determinant Analysis process enables health managers and frontline health workers to readily identify gaps, undertake a causal analysis of the barriers and identify solutions. It garners a data driven approach to implementation even at the lowest level.
Study limitation
The purpose of the study was to assess nutrition services and therefore role of service providers at the basic level (street level bureaucrats) is essential and should have been involved in the assessment. However, critical issues from the basic level were captured by regional officers who work directly with these street level bureaucrats. In addition, the Ten Determinant Model used for the assessment did not explicitly capture indicators on policy, legal, social norms and budget-related factors that shape the determinants of health service coverage. However, these cross-cutting factors were systematically considered as part of analyzing each identified bottleneck during the causal analysis.
Overall in Ghana, there were gaps and insufficient coverage for the six Lancet nutrition specific interventions assessed. Inadequate pre-service and in-service training for staff, low prioritization and coordination (at higher levels) and weak integration of services (at lower levels) were key barriers to nutrition coverage in Ghana. Data driven analysis and planning based on proven nutritional interventions demonstrated gaps and barriers and garnered workable strategies (framework to guide implementation) to improve nutrition services.
Specific recommendations for improving nutrition services include, districts, sub-districts and community level systems being supported with basic commodities to provide the full complement of services. Involvement of all health care workers at districts, sub-districts and community levels and community based volunteers, as well as involvement of health facility managers, stakeholders and partners will be key. Dissemination of all existing and new policies and field guides to the lower levels will be essential. National and sub-national levels should improve data validation activities through regular monitoring and coordination.
Abbreviations
Community based volunteers
Community Health Workers
Community-based Health Planning Services
District Health Information Management System
Exclusive breast feeding
Iron and Folate Supplementation
Infant and young child feeding
Severe acute malnutrition
United Nations Children Fund
Vitamin A Supplementation
World Food Programme
World Health Organization
UNICEF, World Health Organization & World Bank. UNICEF–WHO–the world bank: joint child malnutrition estimates. New York/Geneva/Washington: UNICEF, WHO and World Bank; 2012.
Google Scholar
Headey DD. Developmental drivers of nutritional change: a cross-country analysis. World Dev. 2013;42:76–88.
Article Google Scholar
Black RE, Victora CG, Walker SP, the Maternal and Child Nutrition Study Group. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013. published online June 6. http://dx.doi.org/ 10.1016/S0140-6736(13)60937-X .
Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, Ezzati M, Mathers C, Rivera J. Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. 2008;371:243–60. doi: 10.1016/S0140-6736(07)61690-0 .
Article PubMed Google Scholar
Edmond KM, Zandoh C, Quigley MA, Amenga-Etego S, Owusu-Agyei S, Kirkwood BR. Delayed breastfeeding initiation increases risk of neonatal mortality. Pediatrics. 2006;117:e380–386. doi: 10.1542/peds.2005-1496 .
Bhutta ZA, Das JK, Rizvi A, et al., The Lancet Nutrition Interventions Review Group, and the Maternal and Child Nutrition Study Group. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet. 2013. published online June 6. http://dx. doi.org/ 10.1016/S0140-6736(13)60996-4 . Accessed 10 July 2016.
Victora CG, Adair L, Fall C, Hallal PC, Martorell R, Richter L, Sachdev HS. Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371:340–57. doi: 10.1016/S0140-6736(07)61692-4 .
Article CAS PubMed PubMed Central Google Scholar
Penny ME. In: Walker WA, Watkins JB, Duggan C, editors. Protein–energy malnutrition: pathophysiology, clinical consequences and treatment in Nutrition in Pediatrics. Thirdth ed. Hamilton: BC Decker; 2003. p. 128–31.
Frongillo EA, de Onis M, Hanson KM. Socioeconomic and demographic factors are associated with worldwide patterns of stunting and wasting of children. J Nutr. 1997;127(12):2302–9.
CAS PubMed Google Scholar
Service Ghana Statistical. Ghana statistical service, Ghana health service (GHS), & ICF macro. In: Ghana demographic and health survey 2014 Accra. Ghana: Author; 2014.
Ghana Statistical Service. Ghana multiple indicator cluster survey with an enhanced malaria module and biomarker, final report. Ghana: Accra; 2011.
Ministry of Health. National nutrition policy of Ghana. Ministry Of Health, Accra: Author; 2013.
Ministry of Health. Under Five’s child health policy: 2007–2015. Ministry Of Health, Accra: Author; 2015.
Bhutta ZA, Ahmed T, Black RE, Cousens S, Dewey K, Giugliani E, Haider BA, Kirkwood B, Morris SS, Sachdev HP, et al. What works? Interventions for maternal and child undernutrition and survival. Lancet. 2008;371:417–40. doi: 10.1016/S0140-6736(07)61693-6 .
The Lancet Series-Maternal and Child Nutrition, 2013. http://www.thelancet.com/series/maternal-and-child-nutrition . Accessed 10 July 2016.
Creswell JW. Research design: qualitative, quantitative, and mixed methods approaches. 4th ed. USA: Sage Publications; 2014.
O’Connell T, Sharkey A. Reaching universal health coverage through district health system strengthening: using a modified tanahashi model sub-nationally to attain equitable and effective coverage. In: Maternal, newborn and child health working paper. New York: UNICEF; 2013.
Tanahashi T. Health service coverage and its evaluation. Bull World Health Organ. 1978;56(2):295–303.
CAS PubMed PubMed Central Google Scholar
Ghana Statistical Service. Ghana Multiple Indicator Cluster Survey with an Enhanced Malaria Module and Biomarker, Final Report. Accra: Ghana Statistical Service; 2011.
Ghana Statistical Service. ORC macro: Ghana demographic and health survey 2014. Maryland: GSS/ORC Macro; 2014.
Bezanson K, Isenman P. Scaling up nutrition: a framework for action. Food Nutr Bull. 2010;31:178–86.
Download references
Acknowledgement
A special gratitude is extended to all who contributed towards this process. Acknowledgement is specifically made of the support from UNICEF, and officers and staff of Family Health Division of the Ghana Health Service. We acknowledge the contribution of all the regional directors of health and national and international facilitators, for the effort expended in making the assessment successful.
No source of funding was available for the research.
Availability of data and materials
Available Data used for the analysis and assessment have been included and presented as a supplementary material during submission.
Authors' contributions
AEY, LKS and AOY developed the concept, AEY, and LKS are members of the National Determinant Analysis Facilitation Team for Ghana Health Service and UNICEF and were involved in the analysis in Ghana. AEY, AOY, PKA, EOA, LKS, ABM, LS and VN contributed to the writing and reviewing of various sections of the manuscript. All the authors reviewed the final version of the manuscript before submission. All authors read and approved the final manuscript.
Competing interests
The authors declare no competing interest. The views expressed in this paper are those of the authors. No official endorsement by the Ministry of Health of Ghana/Ghana Health Service is intended or should be inferred.
Consent for publication
Not applicable
Ethics approval and consent to participate
All data used were aggregated data at regional and national and had no link to individuals. In all cases, documentations and computerized records were kept secure and accessible to persons directly involved in the analysis. The Ghana Health Service Ethics Review Committee and office of the Policy, Planning, Monitoring and Evaluation Division of the Ghana Health Service gave approval for documentation and dissemination of the Determinant Analysis process in Ghana.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and affiliations.
Department of Community Health, School of Public Health, College of Health Sciences, University of Ghana, Room 46, P. O. Box 4236, Accra, Ghana
A.E. Yawson
Family Health Division, Ghana Health Service, Accra, Ghana
E.O. Amoaful & P.K. Aboagye
New Juabeng Municipal Health Directorate, Ghana Health Service, Koforidua, Ghana
L.K. Senaya
Department of Child Health, Korle-Bu Teaching Hospital, Accra, Ghana
A.O. Yawson
UNICEF Country Office, Accra, Ghana
A.B. Mahama, L. Selenje & V. Ngongalah
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to A.E. Yawson .
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License ( http://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated.
Reprints and permissions
About this article
Cite this article.
Yawson, A., Amoaful, E., Senaya, L. et al. The lancet series nutritional interventions in Ghana: a determinants analysis approach to inform nutrition strategic planning. BMC Nutr 3 , 27 (2017). https://doi.org/10.1186/s40795-017-0147-1
Download citation
Received : 19 August 2016
Accepted : 10 March 2017
Published : 15 March 2017
DOI : https://doi.org/10.1186/s40795-017-0147-1
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Determinants Analysis
- Health planning
BMC Nutrition
ISSN: 2055-0928
- General enquiries: [email protected]
- Monday, May 20, 2024
- About Ghana News Agency
- GNA Leadership
- GNA Podcast
- Subscription
FETE project to make recommendations for improved nutrition in urban poor
Malnutrition is described as an imbalance between the nutrients one’s body needs to function and the nutrients it gets.
Dr Rose Omari, the Principal Investigator of FETE, who was speaking at the opening of a stakeholder’s workshop, said State and non-State actors had been implementing initiatives on nutrition, but challenges in the sector lingered hence the need to identify the root causes and make recommendations.
The Science and Technology Policy Research Institute, Council for Scientific and Industrial Research (CSIR-STEPRI) and partners from Tanzania, South Africa, Malaysia and Germany are implementing the project.
South Shiashie, Teshie Old Town, New Fadama, Kotobabi, Nungua-Zongo, Agbogbloshie, Osu Alata, Glefe and Nima will benefit from the project.
The workshop sought to establish a network of stakeholders, understand their roles and expectations, and foster a common understanding of the challenges and opportunities.
Dr Omari stated that the project would explore opportunities and develop solutions to shape the food environments to drive nutritious food consumption for better health outcomes.
She noted that increased consumption of diets high in sugar, salt, fat, refined starch-based foods had contributed to the increasing burden of obesity and diet-related non-communicable diseases such as diabetes, hypertension, strokes, cardiovascular diseases and cancer, which demand urgent attention.
D Omari, who is also a Deputy Director, CSIR-STEPRI, said it was critical to examine which interventions were yielding the desired outcomes and adapt and scale them out to other areas both at the national and global levels.
Professor Marian D. Quain, Deputy Director-General, CSIR, raised concerns about the influx of fussy drinks on the market and called for the need to process local fruits into juices, saying “I will rather buy bananas or orange rather than apples”.
She suggested that the collection of a good database on nutritional issues would form a good basis to inform policy makers about the effect on the health system, productivity and economy to trigger policy action.
Dr Geoffrey Asalu, Postdoctoral Researcher, University of Health Allied Sciences, said the project approach would conduct dietary assessments, surveys, participatory geographic information system and focus group discussions to characterise the personal and external domains of food environments.
Share this:
- Health, Pharma & Medtech ›
State of Health
- Malnutrition among children under 5 in Ghana 2018, by indicator
Share of children under five with indicators of malnutrition in Ghana in 2018
Additional Information
Show sources information Show publisher information Use Ask Statista Research Service
January 2019
under 5 years
The source adds the following information: "Stunting refers to a child who is too short for his or her age. Stunting is the failure to grow both physically and cognitively and is the result of chronic or recurrent malnutrition. Wasting refers to a child who is too thin for his or her height. Wasting, or acute malnutrition, is the result of recent rapid weight loss or the failure to gain weight. A child who is moderately or severely wasted has an increased risk of death, but treatment is possible. Overweight refers to a child who is too heavy for his or her height. This form of malnutrition results from expending too few calories for the amount consumed from food and drinks and increases the risk of noncommunicable diseases later in life. Underweight is a composite form of undernutrition that can include elements of stunting and wasting (i.e. an underweight child can have a reduced weight for their age due to being too short for their age and/or being too thin for their height)."
Other statistics on the topic State of health in Ghana
- Coronavirus (COVID-19) cases in Ghana from March 2020 to July 2022
- Cumulative number of COVID-19 vaccine doses administered in Ghana 2022
- Number of malaria cases in Ghana 2010-2022
Health Professionals & Hospitals
- Distribution of health facility ownership in Ghana 2022
- Immediate access to statistics, forecasts & reports
- Usage and publication rights
- Download in various formats
You only have access to basic statistics.
- Instant access to 1m statistics
- Download in XLS, PDF & PNG format
- Detailed references
Business Solutions including all features.
Statistics on " State of health in Ghana "
- Life expectancy at birth in Ghana 2021
- Death rate in Ghana 2021
- Health insurance status in Ghana 2021 by gender
- Availability of basic healthcare facilities in Ghana 2021, by area of residence
- Governmental health spending as a share of GDP in Ghana 2008-2020
- Distribution of current health expenditure in Ghana 2018, by diseases and conditions
- Number of people living with HIV in Ghana 2008-2021
- Number of cancer cases in Ghana 2010-2019
- Number of reported cases of tetanus in Ghana 2002-2022
- Number of reported cases of measles in Ghana 2002-2022
- Poliomyelitis cases reported among children in Ghana 2014-2020
- Number of people undernourished in Africa 2000-2030, by sub-region
- Share of undernourished population in Africa 2022, by region
- Undernourishment in Western African countries 2004-2022
- Tobacco smoking rate in Ghana 2020, by gender
- Tobacco smoking rate among Ghanaian youth 2019, by gender
- Number of smokers in Ghana 2014-2029
- Number of male smokers in Ghana 2001-2029
- Number of female smokers in Ghana 2001-2029
- Vaccination rate of children in Ghana 2022, by type
- Poliomyelitis vaccination coverage among children in Ghana 2018-2020, by type
- Tuberculosis vaccination coverage among children in Ghana 2018-2020
- Measles and rubella vaccination coverage among children in Ghana 2018-2020, by dose
- Hepatitis B immunization coverage among one-year-olds in Ghana 2002-2022
- Yellow fever vaccination coverage among children in Ghana 2018-2020
- Number of HIV/AIDS deaths in Ghana 2001-2020
- Number of deaths from acute hepatitis B in Ghana 2000-2019
- Number of deaths from malaria in Ghana 2010-2022
- Number of deaths from diabetes in Ghana 2010-2019
- Number of deaths from measles in Ghana 2000-2019
- Number of deaths from cervical cancer in Ghana 2000-2019
- Number of deaths from liver cancer in Ghana 2000-2019
Other statistics that may interest you State of health in Ghana
- Basic Statistic Life expectancy at birth in Ghana 2021
- Premium Statistic Death rate in Ghana 2021
- Basic Statistic Health insurance status in Ghana 2021 by gender
- Premium Statistic Availability of basic healthcare facilities in Ghana 2021, by area of residence
- Basic Statistic Distribution of health facility ownership in Ghana 2022
- Premium Statistic Governmental health spending as a share of GDP in Ghana 2008-2020
- Premium Statistic Distribution of current health expenditure in Ghana 2018, by diseases and conditions
- Premium Statistic Number of people living with HIV in Ghana 2008-2021
- Premium Statistic Number of cancer cases in Ghana 2010-2019
- Premium Statistic Number of malaria cases in Ghana 2010-2022
- Premium Statistic Number of reported cases of tetanus in Ghana 2002-2022
- Premium Statistic Number of reported cases of measles in Ghana 2002-2022
- Premium Statistic Poliomyelitis cases reported among children in Ghana 2014-2020
- Basic Statistic Coronavirus (COVID-19) cases in Ghana from March 2020 to July 2022
Malnutrition
- Premium Statistic Number of people undernourished in Africa 2000-2030, by sub-region
- Premium Statistic Share of undernourished population in Africa 2022, by region
- Basic Statistic Undernourishment in Western African countries 2004-2022
- Basic Statistic Malnutrition among children under 5 in Ghana 2018, by indicator
Smoking and tobacco use
- Premium Statistic Tobacco smoking rate in Ghana 2020, by gender
- Basic Statistic Tobacco smoking rate among Ghanaian youth 2019, by gender
- Premium Statistic Number of smokers in Ghana 2014-2029
- Premium Statistic Number of male smokers in Ghana 2001-2029
- Premium Statistic Number of female smokers in Ghana 2001-2029
Vaccination and prevention
- Premium Statistic Vaccination rate of children in Ghana 2022, by type
- Premium Statistic Poliomyelitis vaccination coverage among children in Ghana 2018-2020, by type
- Premium Statistic Tuberculosis vaccination coverage among children in Ghana 2018-2020
- Premium Statistic Measles and rubella vaccination coverage among children in Ghana 2018-2020, by dose
- Premium Statistic Hepatitis B immunization coverage among one-year-olds in Ghana 2002-2022
- Premium Statistic Yellow fever vaccination coverage among children in Ghana 2018-2020
- Basic Statistic Cumulative number of COVID-19 vaccine doses administered in Ghana 2022
- Basic Statistic Number of HIV/AIDS deaths in Ghana 2001-2020
- Premium Statistic Number of deaths from acute hepatitis B in Ghana 2000-2019
- Premium Statistic Number of deaths from malaria in Ghana 2010-2022
- Premium Statistic Number of deaths from diabetes in Ghana 2010-2019
- Premium Statistic Number of deaths from measles in Ghana 2000-2019
- Basic Statistic Number of deaths from cervical cancer in Ghana 2000-2019
- Premium Statistic Number of deaths from liver cancer in Ghana 2000-2019
Further related statistics
- Basic Statistic Percentage of stunted children worldwide under the age of five from 2012 to 2022
- Premium Statistic Colombia: key figures on child deaths due to malnutrition 2012-2016
- Basic Statistic Prevalence of obesity among women by age in France 2013
- Basic Statistic Prevalence of obesity among men by age in France 2013
- Premium Statistic Share of nutritional status among adolescent girls in India 2014
- Basic Statistic Prevalence of obesity in France 2013, by department
- Basic Statistic Current level of health in the U.S. 2014
- Premium Statistic Saint Lucia: food insecurity prevalence 2014-2018, by severity
- Premium Statistic Share of undernourished adult women in rural and urban India 2016
- Premium Statistic South America: food insecurity prevalence 2014-2022, by severity
- Premium Statistic Countries making the slowest progress against child malnutrition, 1990-2010
- Premium Statistic Uruguay: food insecurity prevalence 2014-2022, by severity
- Premium Statistic Malnutrition deaths CARAGA region Philippines 2020, by location
- Basic Statistic Rate of high health status among U.S. women from 2014-2015, by military status
- Premium Statistic Central America: food insecurity prevalence 2014-2020, by severity
Further Content: You might find this interesting as well
- Percentage of stunted children worldwide under the age of five from 2012 to 2022
- Colombia: key figures on child deaths due to malnutrition 2012-2016
- Prevalence of obesity among women by age in France 2013
- Prevalence of obesity among men by age in France 2013
- Share of nutritional status among adolescent girls in India 2014
- Prevalence of obesity in France 2013, by department
- Current level of health in the U.S. 2014
- Saint Lucia: food insecurity prevalence 2014-2018, by severity
- Share of undernourished adult women in rural and urban India 2016
- South America: food insecurity prevalence 2014-2022, by severity
- Countries making the slowest progress against child malnutrition, 1990-2010
- Uruguay: food insecurity prevalence 2014-2022, by severity
- Malnutrition deaths CARAGA region Philippines 2020, by location
- Rate of high health status among U.S. women from 2014-2015, by military status
- Central America: food insecurity prevalence 2014-2020, by severity
- Food & Ecosystems
- Climate Change & Resilience
- Growth & Inclusion
- Where We Work
- Publications
- Data & Tools
- Annual reports
- Our Funders
March-April research journal roundup
Read our roundup of iwmi’s work in april and march 2024..
Forecasting extremes , examining resource governance , establishing conservation , offering sustainab le solutions and ensuring social inclusion are just some of the activities that IWMI researchers have been engaged in during March and April. Read on to discover the full extent of IWMI’s work over the past two months.

Future shifting of annual extreme flows under climate change in the Volta River basin.
The West African Volta River commands a river basin spanning parts of six countries beginning in Burkina Faso and flowing into the Atlantic Ocean via the coast of Ghana. The river enjoys huge hydropower potential, supports a bustling agricultural sector and is rich in biodiversity. Unfortunately, the river is vulnerable to the impacts of climate change with increasing variations in water flow having drastic implications for the frequency of droughts and floods. Published in April, this study co-authored by IWMI’s Sander J. Zwart looks at how timing, seasons and the amount of water flowing in the Volta River Basin might be affected by our rapidly changing climate. Using a method called ‘Circular Statistics’ the research team provided a ‘Mesoscale Hydrologic Model’ with climate data from numerous datasets to see how future river flow might change. The results showed that between 2021-2050 maximum river flow might increase from anywhere between 1%-80% while minimum flow might decrease by 7% – 19%. Understanding the extent of these variations should help stakeholders to prepare for weather extremes.
Read more here.
An evaluation of conventional and nature-based technologies for controlling antibiotic-resistant bacteria and antibiotic-resistant genes in wastewater treatment plants
Disease, death and soaring medical costs are consequences of antibiotic resistance; the result of the evolution of bacteria beyond the efficacy of the antibiotics used to treat them. Preventing the unfortunate repercussions of antibiotic resistance demands that we understand how resistance survives and spreads in water and sewage systems. Without this knowledge, antibiotic resistant bacteria threaten to expose more people to potentially fatal illnesses. Alongside colleagues, IWMI’s Moushumi Hazra has authored a paper reporting on sewage treatment and antibiotic resistance and the need for conventional and nature-based sewage treatment technologies that reduce the number of antibiotic bacteria.
Read more here.
Crop mapping in smallholder farms using unmanned aerial vehicle imagery and geospatial cloud computing infrastructure
Without the contributions of smallholder farmers to the agriculture sector many developing nations would struggle to prevent food insecurity. However, many of these farms and farmers lack the money and tools to produce their best results. Increasing productivity and advancing food security rely on innovative and low-cost agriculture technology. IWMI’s Tafadzwanashe Mabhaudhi is part of a research team which produced a study looking into the use of Unmanned Aerial Vehicles (UAVs) to map land on smallholder farms with the goal of maximizing their potential. Specifically focusing on a program called Google Earth Engine (GEE), the study found that the platform has useful applications for advanced image analysis and could help smallholder farmers to do better.
Development of a composite drought indicator for operational drought monitoring in the MENA region
As temperatures soar across the globe, the result of a rapidly changing climate, regions like MENA are forced to deal with the negative consequences of severe drought events: water scarcity, the exacerbation of poverty, forced displacement and increased vulnerability to disease and malnutrition. This paper, co-authored by IWMI’s Karim Bergaoui, Makaram Blhaj Fraj, Stephen Fragszy and Rachel McDonnell, explores t he benefits of the monthly Composite Drought Indicator (CDI) produced by the Jordanian, Lebanese, Moroccan and Tunisian governments. Intended to help manage drought events by keeping track of anomalies in rainfall, plant life and soil moisture, the CDI supports ‘operational drought management’.
Fostering social inclusion in development-oriented digital food system interventions
How can we ensure that global south digital interventions in farming and food systems do not reinforce existing inequities? Alongside other colleagues, this paper by IWMI’s Simon Langan and Felix Ouku Opola underlines the importance of prioritizing inclusivity for traditionally marginalized groups when it comes to access and usage of emerging digital technology. Digital innovations have the power to enhance participation and productivity in global south food systems. To ensure the advancement of this capacity, the authors believe “a stronger emphasis on inclusivity is required throughout the research for development system.”
Read more here.
Understanding Water Governance in the Central Rift Valley of Ethiopia: Governance Framework, Coherence and Practices
Sustainable water governance is not about quantity over quality, or quality over quantity; we need both to ensure water resources remain sustainable. In the Ethiopian Rift Valley (CRV) formerly rich water resources are coming under increasing strain as the extraction of water intensifies and overpowers the policy in place to protect sustainability in the region. IWMI researcher, Fitsum Hagos, contributed to a study examining the state of CRV water resources and governance which uncovered a lack of coordination between different water resource stakeholders as well as a lack of accountability in decision-making for the region. To reverse this unfortunate series of events the study suggests better coordination, transparency and accountability must be enforced.
Restoring degraded landscapes and sustaining livelihoods: sustainability assessment (cum-review) of integrated landscape management in sub-Saharan Africa.
Combatting land degradation in sub-Saharan Africa can accelerate agricultural productivity, improve social cohesion and advance environmental conservation. Using an Ethiopian and Mali case study approach, this IWMI study measured the ‘sustainability gains’ of Integrated Land Management (ILM) to improve degraded land. Changes in household income, crop growth and soil loss were measured with the sustainable intensification assessment framework (SIAF) and found that ILM has a positive impact on both land and lives in the two African nations.
Read more here.
- natural resource governance
- sustainable solutions
Related Articles
Managing muck and marketing it right.
- Sign up for News
- Whistleblower Hotline
IMAGES
COMMENTS
The health of children in Ghana has improved in recent years. However, the current prevalence rates of malnutrition remain above internationally acceptable levels. This study, therefore, revisits the determinants of child health by using Ghana's Multiple Indicator Cluster Survey to investigate the effect of infant feeding practices on child ...
In Ghana, chronic malnutrition remains a significant public health issue. While Ghana achieved the Millennium Development Goal (MDG) of halving the proportion of children who are underweight and wasted, the reduction in the level of stunting remained off track (UNDP and NDPC Citation 2015). Nearly 19% of children under five are stunted, but ...
there is a decline in the economic growth rate of Ghana [29]. Malnutrition could lead to ... communities living along feeder roads in Ghana. It adopts a qualitative research approach where a total ...
Data is used from the Ghana 2003 Demographic and Health Survey. The results show that malnutrition is related to poverty, maternal education, health care and family planning and regional characteristics. Socioeconomic inequality in malnutrition is mainly associated with poverty, health care use and regional disparities.
Background Understanding the burden and contextual risk factors is critical for developing appropriate interventions to control undernutrition. Methods This study used data from the 2014 Ghana Demographic and Health Survey to estimate the prevalence of underweight, stunting, and wasting. Single multiple logistic regressions were used to identify the factors associated with underweight, wasting ...
There is a wealth of research in Ghana aimed at addressing malnutrition and food insecurity. We briefly highlight three landmark studies which were part of broader cross-national research initiatives and collaborations and yielded findings with the potential to influence practice and policy: 1. the International Lipid-Based Nutrient Supplements ...
Background: Childhood malnutrition contributes to nearly half (45%) of all deaths among children under 5 globally. The United Nations' Sustainable Development Goals (SDGs) aims to end all forms of malnutrition by 2030; however, measuring progress towards these goals is challenging, particularly in countries with emerging economies where nationally-representative data are limited.
This is largely because interventions have not been implemented at scale in all parts of the country in a sustainable and coordinated manner across relevant sectors. Author (s) Ministry of Health, Ghana Health Service. Publication date. November 2016. Languages. English. National Nutrition Policy (PDF, 12 MB) A report on micro-nutrient ...
Ghana: Nutrition Profile. Malnutrition in childhood and pregnancy has many adverse consequences for child survival and long-term well-being. It also has far-reaching consequences for human capital, economic productivity, and national development overall. The consequences of malnutrition should be a significant concern for policymakers in Ghana ...
Ghana: Nutrition Profile. Malnutrition in childhood and pregnancy has many adverse consequences for child survival and long-term well-being. It also has far-reaching consequences for human capital, economic productivity, and national development overall. The consequences of malnutrition should be a significant concern for policymakers in Ghana ...
Studies of malnutrition prevention campaigns for women of childbearing age also had mixed results. In Ghana, vitamin A supplementation was found to increase liver reserves of mothers during the postpartum period, with the effects persisting for at least five months (Citation 72).
However, we posit that Ghana's implementation of the free maternal healthcare policy as well as the community-based health planning and services may account for the low prevalence of stunting with an obese mother. 17 Nonetheless, the results highlight the existing variations in the implementation of maternal and child health nutrition ...
Existing research on the causal relationship between child malnutrition and education outcomes in Ghana is scanty. Our review of the literature points to two main studies by Glewwe and Jacoby (1995) and Ampaabeng and Tan . In the dated Glewwe and Jacoby (1995) study, the authors use instrumental variables and cross-sectional data to deal with ...
Malnutrition is a leading cause of mortality and morbidity among children in low- and middle-income countries. Ghana is one of 36 countries with the highest burden of stunting, globally. The aim of this work is to use data driven planning methods to conduct in-depth analysis on the Lancet series nutrition interventions in Ghana to inform nutritional strategic planning.
Through action research and development partnerships, Africa RISING will create opportunities for ... extension workers, and media professionals to help to address malnutrition in northern Ghana. viii. 1 Why is this booklet needed? Having ideal nutrition is critical for human development and economic growth. However, childhood
This study analyzed the factors affecting stunting and wasting in children 0-59 month's old in. Northern Ghana using secondary data from Feed the Future Northern Ghana survey data. The study found ...
In Ghana, progress to reduce malnutrition has improved, but almost 7 percent of children under 5 are still affected by wasting — the deadliest form of malnutrition. **The Government of Ghana is ...
Malnutrition is described as an imbalance between the nutrients one's body needs to function and the nutrients it gets. Dr Rose Omari, the Principal Investigator of FETE, who was speaking at the opening of a stakeholder's workshop, said State and non-State actors had been implementing initiatives on nutrition, but challenges in the sector lingered hence the need to identify the root causes ...
research-driven agricultural interventions to improve yield that withstand the effect of climate change. This review is aimed to present the food and nutrition security situation ... energy-dense nutrient-poor foods contributing to the burden of malnutrition. In Ghana, 5% (1.5 million) of the population experienced food insecurity in 2018 [10].
Customized Research & Analysis projects: ... Share of children under five with indicators of malnutrition in Ghana in 2018 [Graph], UNICEF, January 15, 2019. [Online]. Available: https://www ...
Read our roundup of IWMI's work in April and March 2024. May 13, 2024. By Luisa Edmond. 4. Forecasting extremes, examining resource governance, establishing conservation, offering sustainable solutions and ensuring social inclusion are just some of the activities that IWMI researchers have been engaged in during March and April.